

A non-invasive continuous and real-time volumetric monitoring in spontaneous breathing subjects based on bioimpedance-ExSpiron®Xi: a validation study in healthy volunteers
- PMID: 38238635
- PMCID: PMC10994998
- DOI: 10.1007/s10877-023-01107-0
A non-invasive continuous and real-time volumetric monitoring in spontaneous breathing subjects based on bioimpedance-ExSpiron®Xi: a validation study in healthy volunteers
Abstract
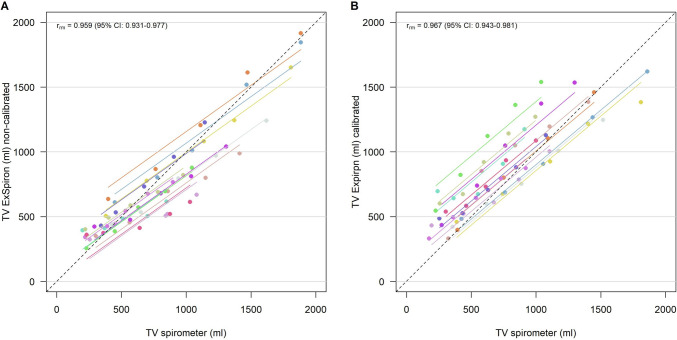
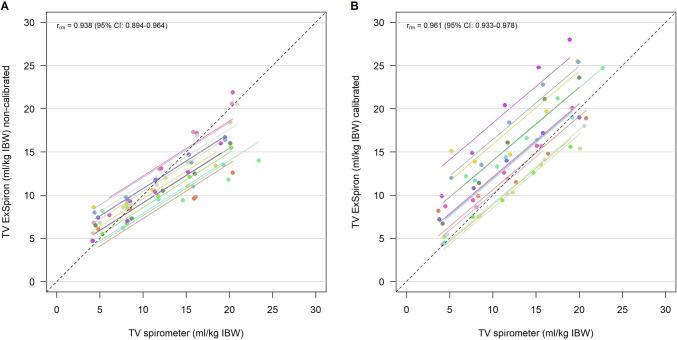
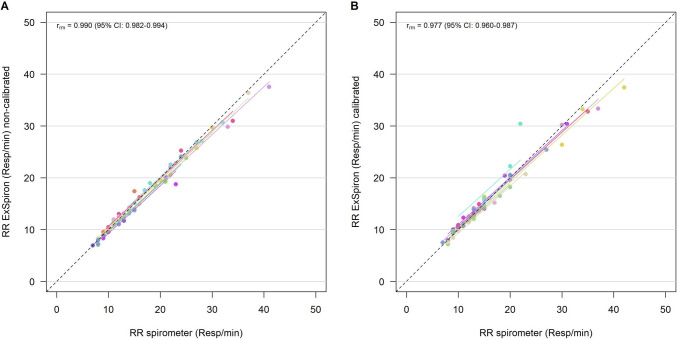
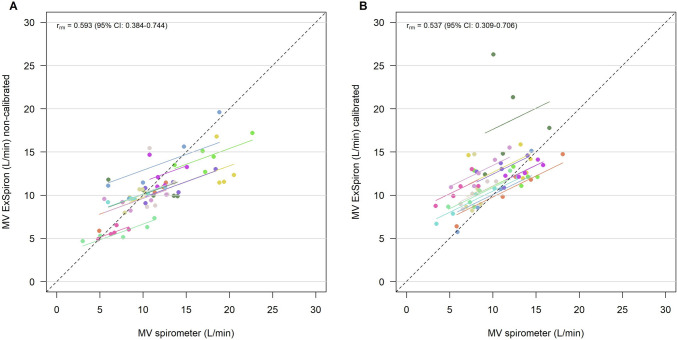
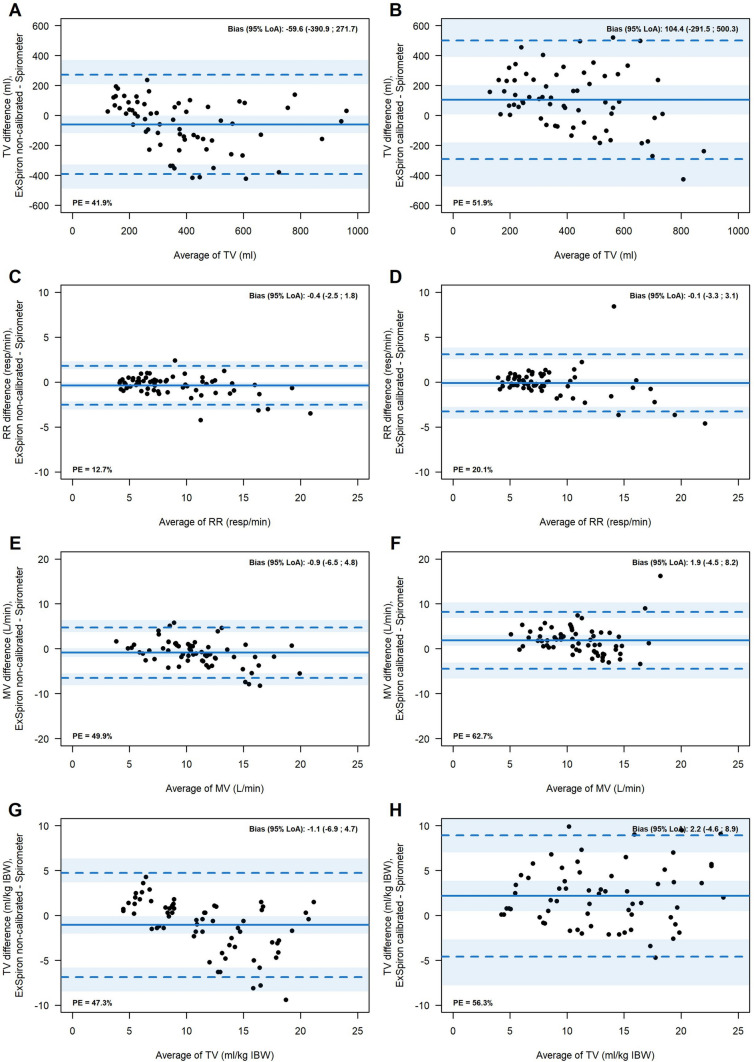
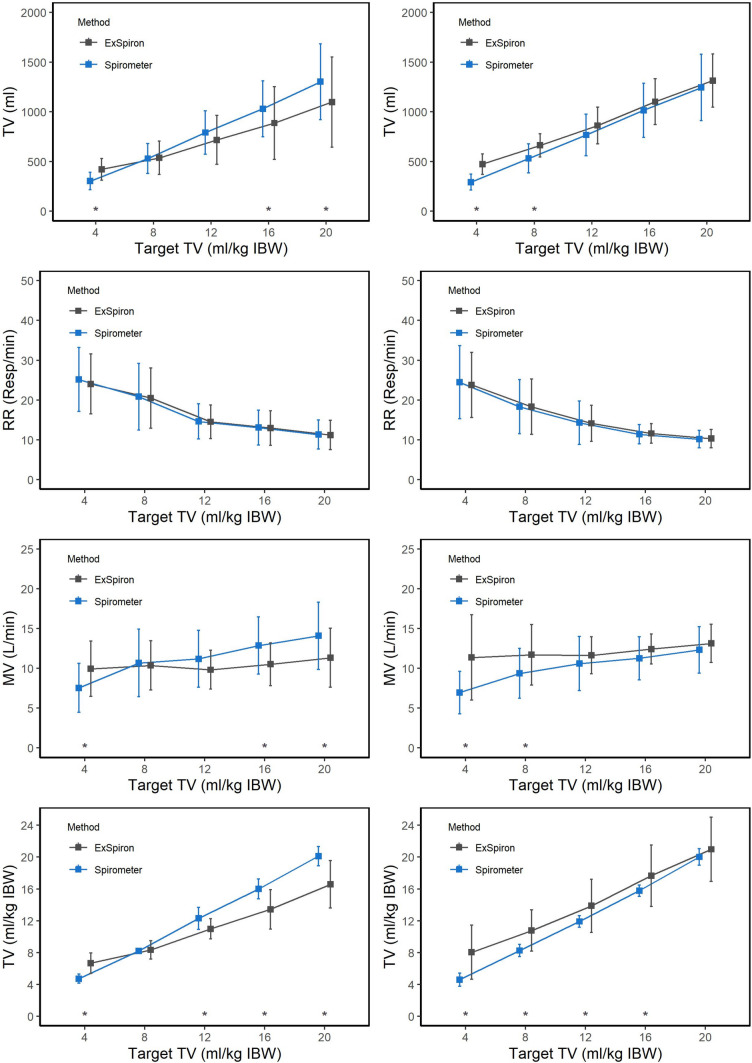
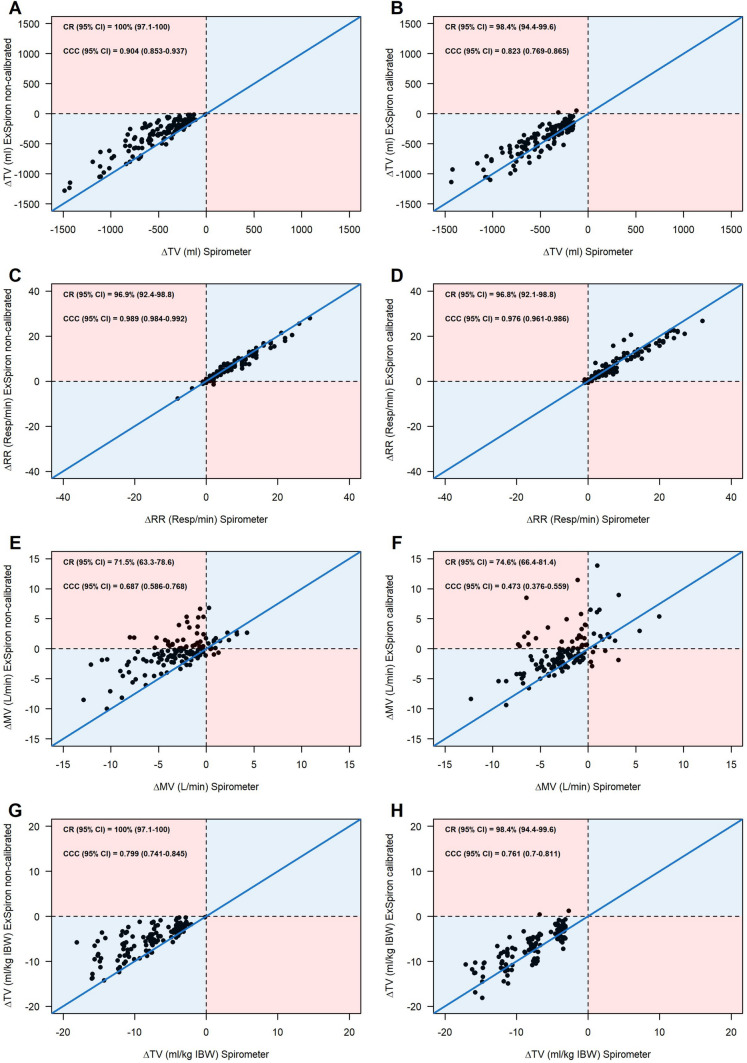
Tidal volume (TV) monitoring breath-by-breath is not available at bedside in non-intubated patients. However, TV monitoring may be useful to evaluate the work of breathing. A non-invasive device based on bioimpedance provides continuous and real-time volumetric tidal estimation during spontaneous breathing. We performed a prospective study in healthy volunteers aimed at evaluating the accuracy, the precision and the trending ability of measurements of ExSpiron®Xi as compared with the gold standard (i.e. spirometry). Further, we explored whether the differences between the 2 devices would be improved by the calibration of ExSpiron®Xi with a pre-determined tidal volume. Analysis accounted for the repeated nature of measurements within each subject. We enrolled 13 healthy volunteers, including 5 men and 8 women. Tidal volume, TV/ideal body weight (IBW) and respiratory rate (RR) measured with spirometer (TVSpirometer) and with ExSpiron®Xi (TVExSpiron) showed a robust correlation, while minute ventilation (MV) showed a weak correlation, in both non/calibrated and calibrated steps. The analysis of the agreement showed that non-calibrated TVExSpiron underestimated TVspirometer, while in the calibrated steps, TVExSpiron overestimated TVspirometer. The calibration procedure did not reduce the average absolute difference (error) between TVSpirometer and TVExSpiron. This happened similarly for TV/IBW and MV, while RR showed high accuracy and precision. The trending ability was excellent for TV, TV/IBW and RR. The concordance rate (CR) was >95% in both calibrated and non-calibrated measurements. The trending ability of minute ventilation was limited. Absolute error for both calibrated and not calibrated values of TV, TV/IBW and MV accounting for repeated measurements was variably associated with BMI, height and smoking status. Conclusions: Non-invasive TV, TV/IBW and RR estimation by ExSpiron®Xi was strongly correlated with tidal ventilation according to the gold standard spirometer technique. This data was not confirmed for MV. The calibration of the device did not improve its performance. Although the accuracy of ExSpiron®Xi was mild and the precision was limited for TV, TV/IBW and MV, the trending ability of the device was strong specifically for TV, TV/IBW and RR. This makes ExSpiron®Xi a non-invasive monitoring system that may detect real-time tidal volume ventilation changes and then suggest the need to better optimize the patient ventilatory support.
Keywords: Bioimpedance; Healthy volunteers; Non-invasive monitoring; Non-invasive respiratory support; Non-invasive ventilation; Respiratory failure; Tidal volume.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The Evaluation of a Noninvasive Respiratory Volume Monitor in Mechanically Ventilated Neonates and Infants.Anesth Analg. 2022 Jan 1;134(1):141-148. doi: 10.1213/ANE.0000000000005562. Anesth Analg. 2022. PMID: 33929346
-
The Evaluation of a Noninvasive Respiratory Volume Monitor in Pediatric Patients Undergoing General Anesthesia.Anesth Analg. 2017 Dec;125(6):1913-1919. doi: 10.1213/ANE.0000000000002029. Anesth Analg. 2017. PMID: 28759491 Clinical Trial.
-
A Comparison of Measurements of Change in Respiratory Status in Spontaneously Breathing Volunteers by the ExSpiron Noninvasive Respiratory Volume Monitor Versus the Capnostream Capnometer.Anesth Analg. 2017 Jan;124(1):120-126. doi: 10.1213/ANE.0000000000001395. Anesth Analg. 2017. PMID: 27384980
-
Special article: evaluation of a novel noninvasive respiration monitor providing continuous measurement of minute ventilation in ambulatory subjects in a variety of clinical scenarios.Anesth Analg. 2013 Jul;117(1):91-100. doi: 10.1213/ANE.0b013e3182918098. Epub 2013 Jun 3. Anesth Analg. 2013. PMID: 23733842
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
Cited by
-
Assessing inspiratory drive and effort in critically ill patients at the bedside.Crit Care. 2025 Jul 31;29(1):339. doi: 10.1186/s13054-025-05526-0. Crit Care. 2025. PMID: 40745324 Free PMC article. Review.
-
Day-to-Day Variability in Measurements of Respiration Using Bioimpedance from a Non-Standard Location.Sensors (Basel). 2024 Jul 16;24(14):4612. doi: 10.3390/s24144612. Sensors (Basel). 2024. PMID: 39066010 Free PMC article.
-
Monitoring patients with acute respiratory failure during non-invasive respiratory support to minimize harm and identify treatment failure.Crit Care. 2025 Apr 9;29(1):147. doi: 10.1186/s13054-025-05369-9. Crit Care. 2025. PMID: 40205493 Free PMC article. Review.
-
Effect of Helmet CPAP on Tidal Volume Assessed by Bioelectrical Impedance.Respir Care. 2024 Sep 26;69(10):1332-1335. doi: 10.4187/respcare.11959. Respir Care. 2024. PMID: 39043426 No abstract available.
References
-
- Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–1308. doi: 10.1056/NEJM200005043421801. - DOI - PubMed
-
- Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, Adhikari NKJ, Amato MBP, Branson R, Brower RG, Ferguson ND, Gajic O, Gattinoni L, Hess D, Mancebo J, Meade MO, McAuley DF, Pesenti A, Ranieri VM, Rubenfeld GD, Rubin E, Seckel M, Slutsky AS, Talmor D, Thompson BT, Wunsch H, Uleryk E, Brozek J, Brochard LJ, American Thoracic Society, European Society of Intensive Care Medicine, and Society of Critical Care Medicine An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine Clinical Practice guideline: mechanical ventilation in adult patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 2017;195(9):1253–1263. doi: 10.1164/rccm.201703-0548ST. - DOI - PubMed
-
- Carteaux G, Millán-Guilarte T, De Prost N, Razazi K, Abid S, Thille AW, Schortgen F, Brochard L, Brun-Buisson C, Mekontso DA. Failure of noninvasive ventilation for de novo acute hypoxemic respiratory failure: role of tidal volume. Crit Care Med. 2016;44(2):282–290. doi: 10.1097/CCM.0000000000001379. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
