

Cell-free DNA levels associate with COPD exacerbations and mortality
- PMID: 38238743
- PMCID: PMC10797855
- DOI: 10.1186/s12931-023-02658-1
Cell-free DNA levels associate with COPD exacerbations and mortality
Abstract
The question addressed by the study: Good biological indicators capable of predicting chronic obstructive pulmonary disease (COPD) phenotypes and clinical trajectories are lacking. Because nuclear and mitochondrial genomes are damaged and released by cigarette smoke exposure, plasma cell-free mitochondrial and nuclear DNA (cf-mtDNA and cf-nDNA) levels could potentially integrate disease physiology and clinical phenotypes in COPD. This study aimed to determine whether plasma cf-mtDNA and cf-nDNA levels are associated with COPD disease severity, exacerbations, and mortality risk.
Materials and methods: We quantified mtDNA and nDNA copy numbers in plasma from participants enrolled in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE, n = 2,702) study and determined associations with relevant clinical parameters.
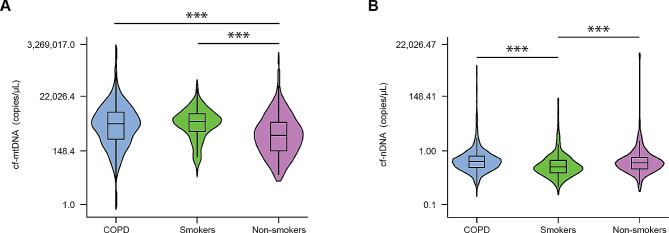
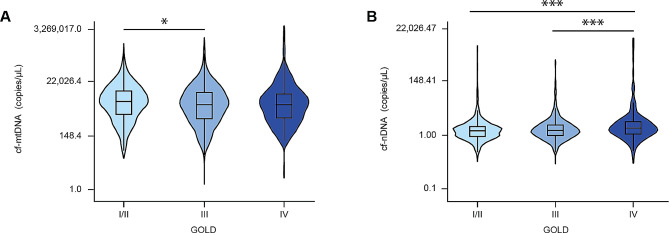
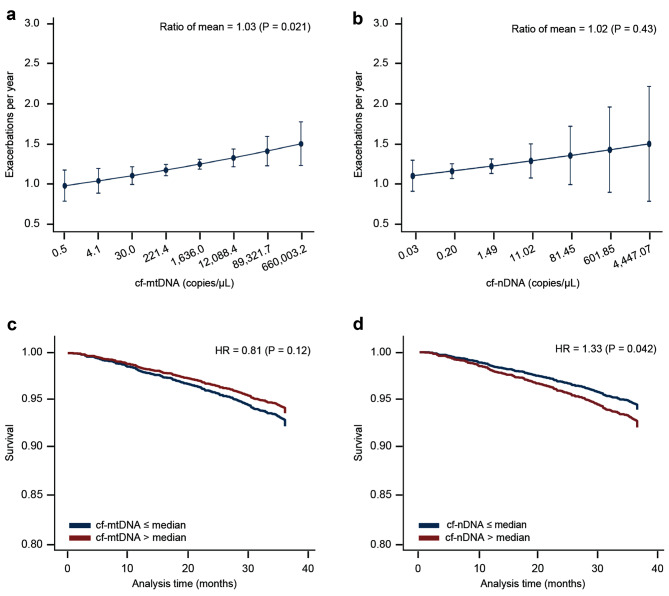
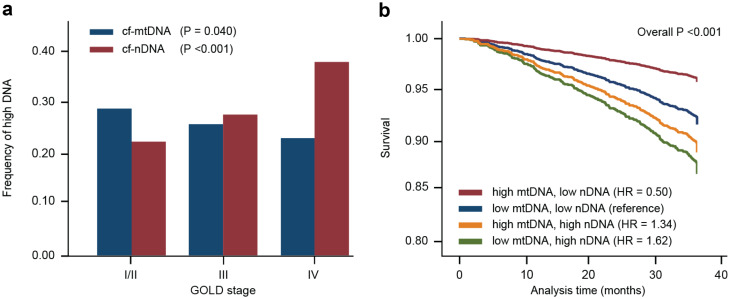
Results: Of the 2,128 participants with COPD, 65% were male and the median age was 64 (interquartile range, 59-69) years. During the baseline visit, cf-mtDNA levels positively correlated with future exacerbation rates in subjects with mild/moderate and severe disease (Global Initiative for Obstructive Lung Disease [GOLD] I/II and III, respectively) or with high eosinophil count (≥ 300). cf-nDNA positively associated with an increased mortality risk (hazard ratio, 1.33 [95% confidence interval, 1.01-1.74] per each natural log of cf-nDNA copy number). Additional analysis revealed that individuals with low cf-mtDNA and high cf-nDNA abundance further increased the mortality risk (hazard ratio, 1.62 [95% confidence interval, 1.16-2.25] per each natural log of cf-nDNA copy number).
Answer to the question: Plasma cf-mtDNA and cf-nDNA, when integrated into quantitative clinical measurements, may aid in improving COPD severity and progression assessment.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Urinary cell-free mitochondrial and nuclear deoxyribonucleic acid correlates with the prognosis of chronic kidney diseases.BMC Nephrol. 2019 Oct 28;20(1):391. doi: 10.1186/s12882-019-1549-x. BMC Nephrol. 2019. PMID: 31660901 Free PMC article.
-
Probing the diagnostic values of plasma cf-nDNA and cf-mtDNA for Parkinson's disease and multiple system atrophy.Front Neurosci. 2024 Dec 2;18:1488820. doi: 10.3389/fnins.2024.1488820. eCollection 2024. Front Neurosci. 2024. PMID: 39687490 Free PMC article.
-
Extracellular Release of Mitochondrial DNA: Triggered by Cigarette Smoke and Detected in COPD.Cells. 2022 Jan 22;11(3):369. doi: 10.3390/cells11030369. Cells. 2022. PMID: 35159179 Free PMC article.
-
Anti-IL-5 therapies for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2020 Dec 8;12(12):CD013432. doi: 10.1002/14651858.CD013432.pub2. Cochrane Database Syst Rev. 2020. PMID: 33295032 Free PMC article.
-
Tailored or adapted interventions for adults with chronic obstructive pulmonary disease and at least one other long-term condition: a mixed methods review.Cochrane Database Syst Rev. 2021 Jul 26;7(7):CD013384. doi: 10.1002/14651858.CD013384.pub2. Cochrane Database Syst Rev. 2021. PMID: 34309831 Free PMC article.
Cited by
-
Exploring the Common Genetic Underpinnings of Chronic Pulmonary Disease and Esophageal Carcinoma Susceptibility.J Cancer. 2024 Apr 29;15(11):3406-3417. doi: 10.7150/jca.95437. eCollection 2024. J Cancer. 2024. PMID: 38817868 Free PMC article.
-
The role of the cGAS-STING pathway in chronic pulmonary inflammatory diseases.Front Med (Lausanne). 2024 Oct 30;11:1436091. doi: 10.3389/fmed.2024.1436091. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39540037 Free PMC article. Review.
-
Increased levels of circulating cell-free DNA in COVID-19 patients with respiratory failure.Sci Rep. 2024 Jul 29;14(1):17399. doi: 10.1038/s41598-024-68433-4. Sci Rep. 2024. PMID: 39075117 Free PMC article.
-
Mitochondrial DNA signals driving immune responses: Why, How, Where?Cell Commun Signal. 2025 Apr 22;23(1):192. doi: 10.1186/s12964-025-02042-0. Cell Commun Signal. 2025. PMID: 40264103 Free PMC article. Review.
-
Comparative Assessment of Acute Pulmonary Effects Induced by Heat-Not-Burn Tobacco Aerosol Inhalation in a Murine Model.Int J Mol Sci. 2025 Jan 28;26(3):1135. doi: 10.3390/ijms26031135. Int J Mol Sci. 2025. PMID: 39940903 Free PMC article.
References
-
- World Health Organization, Updated who projections of mortality and causes of. death 2016-2060 [Internet]. Updated who projections of mortality and causes of death 2016–2060 2018 [cited 2021 Jun 28].Available from: https://www.who.int/healthinfo/global_burden_disease/projections_method.....
-
- 2020 GLOBAL Global Initiative for chronic obstructive lung disease, strategy for prevention, diagnosis and management of COPD [Internet]. 2020 [cited 2021 Jun 29].Available from: https://goldcopd.org/gold-reports/.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
