

Time-Controlled Adaptive Ventilation (TCAV): a personalized strategy for lung protection
- PMID: 38238778
- PMCID: PMC10797864
- DOI: 10.1186/s12931-023-02615-y
Time-Controlled Adaptive Ventilation (TCAV): a personalized strategy for lung protection
Abstract
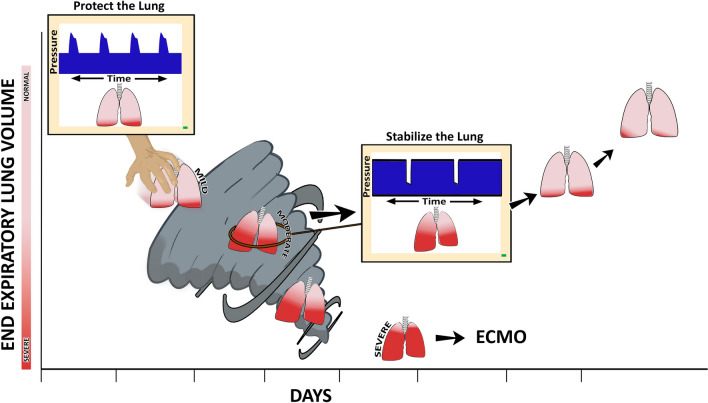
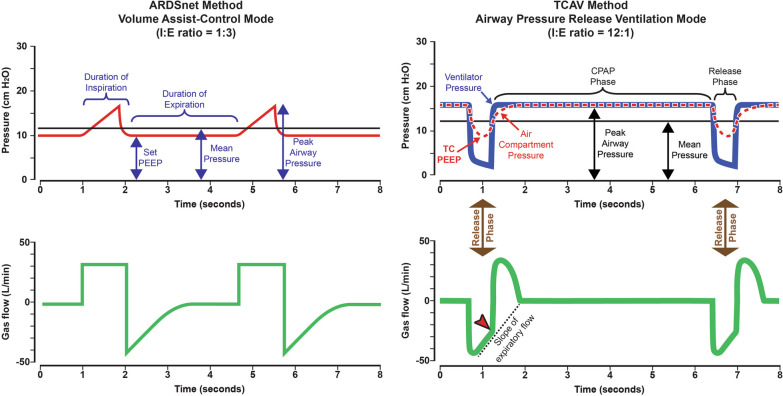
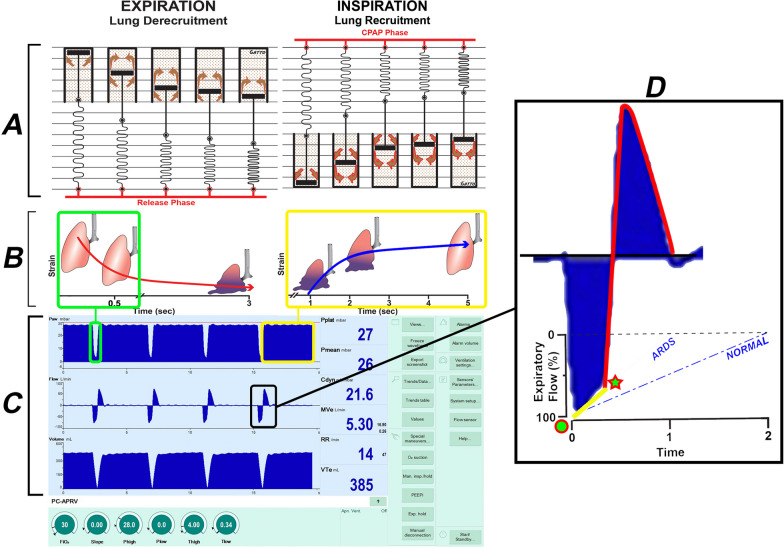
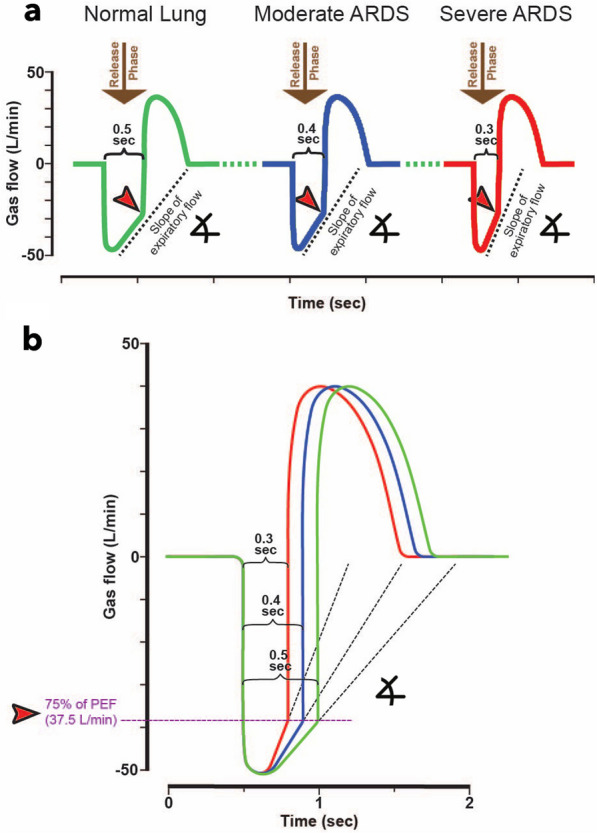
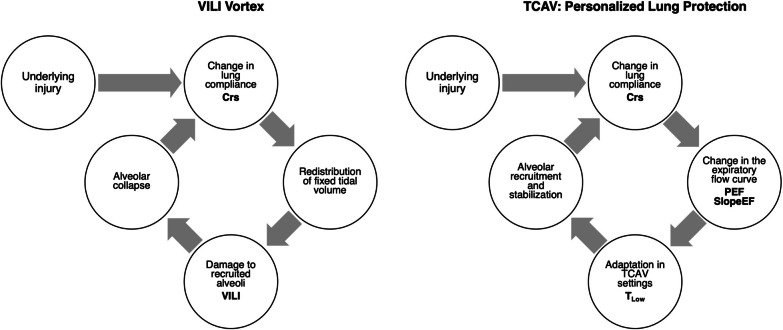
Acute respiratory distress syndrome (ARDS) alters the dynamics of lung inflation during mechanical ventilation. Repetitive alveolar collapse and expansion (RACE) predisposes the lung to ventilator-induced lung injury (VILI). Two broad approaches are currently used to minimize VILI: (1) low tidal volume (LVT) with low-moderate positive end-expiratory pressure (PEEP); and (2) open lung approach (OLA). The LVT approach attempts to protect already open lung tissue from overdistension, while simultaneously resting collapsed tissue by excluding it from the cycle of mechanical ventilation. By contrast, the OLA attempts to reinflate potentially recruitable lung, usually over a period of seconds to minutes using higher PEEP used to prevent progressive loss of end-expiratory lung volume (EELV) and RACE. However, even with these protective strategies, clinical studies have shown that ARDS-related mortality remains unacceptably high with a scarcity of effective interventions over the last two decades. One of the main limitations these varied interventions demonstrate to benefit is the observed clinical and pathologic heterogeneity in ARDS. We have developed an alternative ventilation strategy known as the Time Controlled Adaptive Ventilation (TCAV) method of applying the Airway Pressure Release Ventilation (APRV) mode, which takes advantage of the heterogeneous time- and pressure-dependent collapse and reopening of lung units. The TCAV method is a closed-loop system where the expiratory duration personalizes VT and EELV. Personalization of TCAV is informed and tuned with changes in respiratory system compliance (CRS) measured by the slope of the expiratory flow curve during passive exhalation. Two potentially beneficial features of TCAV are: (i) the expiratory duration is personalized to a given patient's lung physiology, which promotes alveolar stabilization by halting the progressive collapse of alveoli, thereby minimizing the time for the reopened lung to collapse again in the next expiration, and (ii) an extended inspiratory phase at a fixed inflation pressure after alveolar stabilization gradually reopens a small amount of tissue with each breath. Subsequently, densely collapsed regions are slowly ratcheted open over a period of hours, or even days. Thus, TCAV has the potential to minimize VILI, reducing ARDS-related morbidity and mortality.
Keywords: APRV; ARDS; ARMA; Acute respiratory distress syndrome; Alveolar opening and collapse time constants; Driving pressure; Dynamic alveolar mechanics; Open lung approach; Regional alveolar instability; Stress-multipliers; TCAV; Tidal volume; VILI; Ventilator-induced lung injury; Viscoelastic.
© 2024. The Author(s).
Conflict of interest statement
MKS has received a Research Grant and GFN an Unrestricted Educational Grant from Dräger Medical Systems, Inc. GFN, MKS have presented and received honoraria and/or travel reimbursement at event(s) sponsored by Dräger Medical Systems, Inc., outside of the published work. GFN, MKS, have lectured for Intensive Care On-line Network, Inc. (ICON). NMH is the founder of ICON, of which PLA is an employee. NMH holds patents on a method of initiating, managing and/or weaning airway pressure release ventilation, as well as controlling a ventilator in accordance with the same. DWK and JH are co-founders and shareholders of OscillaVent, Inc., and are co-inventors on a patent involving multi-frequency oscillatory ventilation. DWK and JH also receive research support from ZOLL Medical Corporation, and DWK is a consultant for Lungpacer Medical, Inc. JHTB is a consultant to and shareholder of OscillaVent, Inc., and has two patents pending in the field of MV. The authors maintain that industry had no role in the design and conduct of the study; the collection, management, analysis, or interpretation of the data; nor the preparation, review, or approval of the manuscript.
Figures
Similar articles
-
First Stabilize and then Gradually Recruit: A Paradigm Shift in Protective Mechanical Ventilation for Acute Lung Injury.J Clin Med. 2023 Jul 12;12(14):4633. doi: 10.3390/jcm12144633. J Clin Med. 2023. PMID: 37510748 Free PMC article. Review.
-
Prevention and treatment of acute lung injury with time-controlled adaptive ventilation: physiologically informed modification of airway pressure release ventilation.Ann Intensive Care. 2020 Jan 6;10(1):3. doi: 10.1186/s13613-019-0619-3. Ann Intensive Care. 2020. PMID: 31907704 Free PMC article. Review.
-
A Physiologically Informed Strategy to Effectively Open, Stabilize, and Protect the Acutely Injured Lung.Front Physiol. 2020 Mar 19;11:227. doi: 10.3389/fphys.2020.00227. eCollection 2020. Front Physiol. 2020. PMID: 32265734 Free PMC article. Review.
-
Airway pressure release ventilation for lung protection in acute respiratory distress syndrome: an alternative way to recruit the lungs.Curr Opin Crit Care. 2024 Feb 1;30(1):76-84. doi: 10.1097/MCC.0000000000001123. Epub 2023 Dec 1. Curr Opin Crit Care. 2024. PMID: 38085878 Review.
-
Physiology in Medicine: Understanding dynamic alveolar physiology to minimize ventilator-induced lung injury.J Appl Physiol (1985). 2017 Jun 1;122(6):1516-1522. doi: 10.1152/japplphysiol.00123.2017. Epub 2017 Apr 6. J Appl Physiol (1985). 2017. PMID: 28385915 Free PMC article. Review.
Cited by
-
Comparison of airway pressure release ventilation (APRV) versus biphasic positive airway pressure (BIPAP) ventilation in COVID-19 associated ARDS using transpulmonary pressure monitoring.BMC Anesthesiol. 2025 Feb 1;25(1):52. doi: 10.1186/s12871-025-02904-7. BMC Anesthesiol. 2025. PMID: 39893363 Free PMC article.
-
A narrative review on the future of ARDS: evolving definitions, pathophysiology, and tailored management.Crit Care. 2025 Feb 24;29(1):88. doi: 10.1186/s13054-025-05291-0. Crit Care. 2025. PMID: 39994815 Free PMC article. Review.
-
Current practice of using the airway pressure release ventilation mode in acute respiratory distress syndrome patients among respiratory therapists in Saudi Arabia.SAGE Open Med. 2025 Jan 16;13:20503121241312941. doi: 10.1177/20503121241312941. eCollection 2025. SAGE Open Med. 2025. PMID: 39839159 Free PMC article.
-
Imaging the Lung in ARDS: A Primer.Respir Care. 2024 Jul 24;69(8):1011-1024. doi: 10.4187/respcare.12061. Respir Care. 2024. PMID: 39048146 Free PMC article. Review.
References
-
- Laffey JG, Bellani G, Pham T, Fan E, Madotto F, Bajwa EK, Brochard L, Clarkson K, Esteban A, Gattinoni L, et al. Potentially modifiable factors contributing to outcome from acute respiratory distress syndrome: the LUNG SAFE study. Intensive Care Med. 2016;42:1865–1876. doi: 10.1007/s00134-016-4571-5. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
