

Case report: Clinically mild encephalitis/encephalopathy with a reversible splenial lesion: an autopsy case
- PMID: 38239318
- PMCID: PMC10794512
- DOI: 10.3389/fneur.2023.1322302
Case report: Clinically mild encephalitis/encephalopathy with a reversible splenial lesion: an autopsy case
Abstract
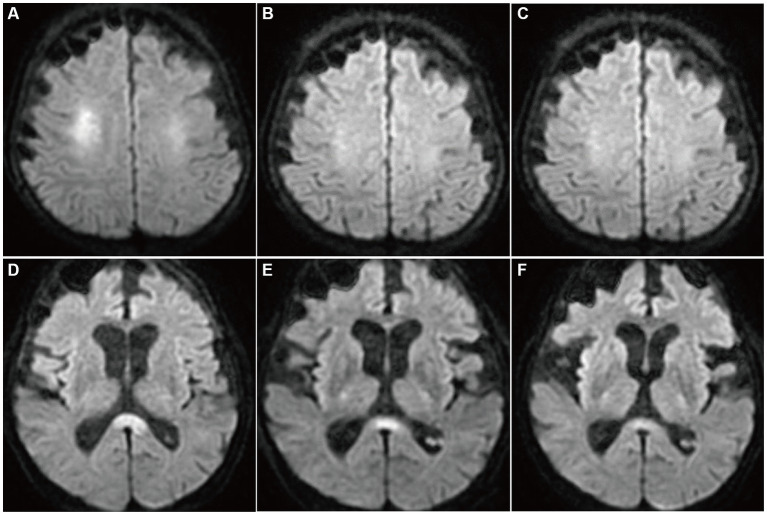
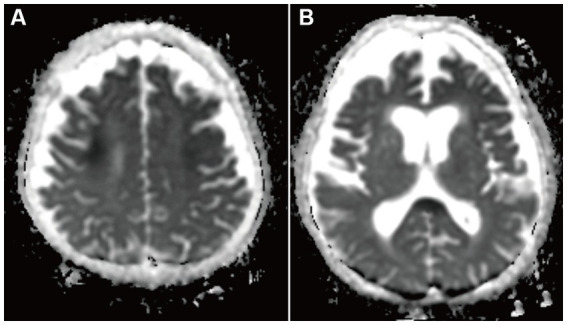
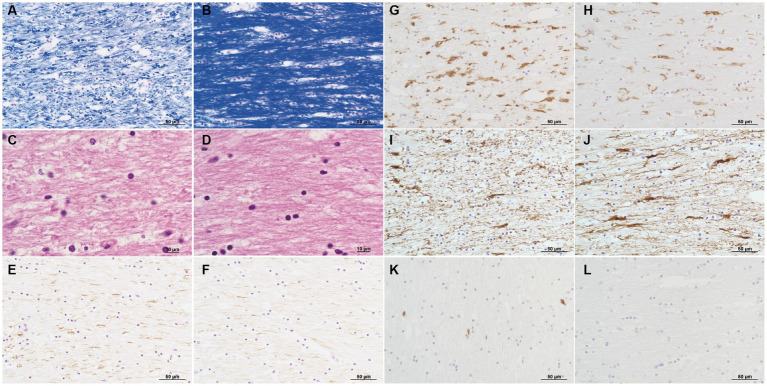
Clinically mild encephalitis/encephalopathy with a reversible splenial lesion is a clinicoradiological syndrome characterized by transient neuropsychiatric symptoms and hyperintensity of the splenium of the corpus callosum on diffusion-weighted MRI. Although intramyelinic edema and inflammatory cell infiltration can be predicted by MRI, the pathology of the splenium of the corpus callosum remains unknown. We encountered a case of clinically mild encephalitis/encephalopathy with a reversible splenial lesion and hypoglycemia in a patient who died of sepsis, and an autopsy was performed. The postmortem pathological findings included intramyelinic edema, myelin pallor, loss of fibrous astrocytes, microglial reactions, and minimal lymphocytic infiltration in the parenchyma. Based on these findings, transient demyelination following cytotoxic edema in the splenium of corpus callosum was strongly considered a pathogenesis of "clinically mild encephalitis/encephalopathy with a reversible splenial lesion" associated with hypoglycemia, and it could be generalized for the disease associated with the other causes. As cytotoxic edema could be the central pathology of the disease, the recently proposed term cytotoxic lesions of the corpus callosum may be applicable to this syndrome.
Keywords: autopsy: MRI; clinically mild encephalitis/encephalopathy with reversible splenial lesions; corpus callosum splenium; cytotoxic edema; hypoglycemia.
Copyright © 2024 Hayashi, Ueda, Hayashi, Kawahara, Azuma, Suzuki, Nakaya, Asano, Sato, Miura, Hayashi, Hayashi and Kobayashi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Cytotoxic Lesions of the Corpus Callosum (CLOCCs) Related to Hypoglycemia: Clinical Insights and Pathogenesis.Cureus. 2024 Sep 23;16(9):e69965. doi: 10.7759/cureus.69965. eCollection 2024 Sep. Cureus. 2024. PMID: 39445273 Free PMC article.
-
Mild encephalitis/encephalopathy with a reversible splenial lesion associated with systemic Mycoplasma pneumoniae infection in North America: a case report.J Med Case Rep. 2022 Feb 20;16(1):74. doi: 10.1186/s13256-022-03299-6. J Med Case Rep. 2022. PMID: 35183255 Free PMC article.
-
Mild Encephalopathy/Encephalitis with Reversible Splenial Lesion in a Patient with Salmonella typhi Infection: An Unusual Presentation with Excellent Prognosis.Indian J Crit Care Med. 2019 Dec;23(12):584-586. doi: 10.5005/jp-journals-10071-23300. Indian J Crit Care Med. 2019. PMID: 31988550 Free PMC article.
-
Reversible lesion in the splenium of the corpus callosum.Brain Behav. 2019 Nov;9(11):e01440. doi: 10.1002/brb3.1440. Epub 2019 Oct 6. Brain Behav. 2019. PMID: 31588684 Free PMC article. Review.
-
[Clinically mild encephalitis/encephalopathy with a reversible splenial lesion of corpus callosum in a child and literature review].Zhonghua Er Ke Za Zhi. 2014 Mar;52(3):218-22. Zhonghua Er Ke Za Zhi. 2014. PMID: 24824394 Review. Chinese.
Cited by
-
Cytotoxic Lesions of the Corpus Callosum (CLOCCs) Related to Hypoglycemia: Clinical Insights and Pathogenesis.Cureus. 2024 Sep 23;16(9):e69965. doi: 10.7759/cureus.69965. eCollection 2024 Sep. Cureus. 2024. PMID: 39445273 Free PMC article.
-
Case report: Re-evaluating reversibility of cytotoxic lesions of the corpus callosum.Front Neuroimaging. 2025 Feb 17;4:1436931. doi: 10.3389/fnimg.2025.1436931. eCollection 2025. Front Neuroimaging. 2025. PMID: 40034189 Free PMC article.
-
Tuberculous Meningitis in a Child: A Rare Presentation of Cytotoxic Lesion of the Corpus Callosum.Trop Med Infect Dis. 2025 Apr 4;10(4):96. doi: 10.3390/tropicalmed10040096. Trop Med Infect Dis. 2025. PMID: 40278769 Free PMC article.
-
Case report: Rare Guillain-Barré syndrome variants and mild encephalitis/encephalopathy with a reversible splenial lesion as the para-infectious manifestations of SARS-CoV-2 infection.Front Immunol. 2024 Oct 4;15:1458231. doi: 10.3389/fimmu.2024.1458231. eCollection 2024. Front Immunol. 2024. PMID: 39430766 Free PMC article.
-
Mild encephalitis/encephalopathy with reversible corpus callosum lesion associated with listeria infection with meningoencephalitis: a case report.Front Med (Lausanne). 2025 Jul 11;12:1568219. doi: 10.3389/fmed.2025.1568219. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40718417 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials