

Minimally invasive treatment of postoperative fistulas, leakages, and perforations of the upper gastrointestinal tract: a single-center observational study
- PMID: 38239587
- PMCID: PMC10793144
- DOI: 10.5114/wiitm.2023.133838
Minimally invasive treatment of postoperative fistulas, leakages, and perforations of the upper gastrointestinal tract: a single-center observational study
Abstract
Introduction: Most anastomotic leaks in the upper gastrointestinal (GI) tract can be treated with minimally invasive techniques dominated by endoluminal vacuum therapy (EVT) or stent implantation. Chronic leaks often require additional solutions, such as tissue adhesives or cellular growth stimulants.
Aim: To present a treatment strategy for postoperative leakage of upper GI anastomoses with noninvasive procedures.
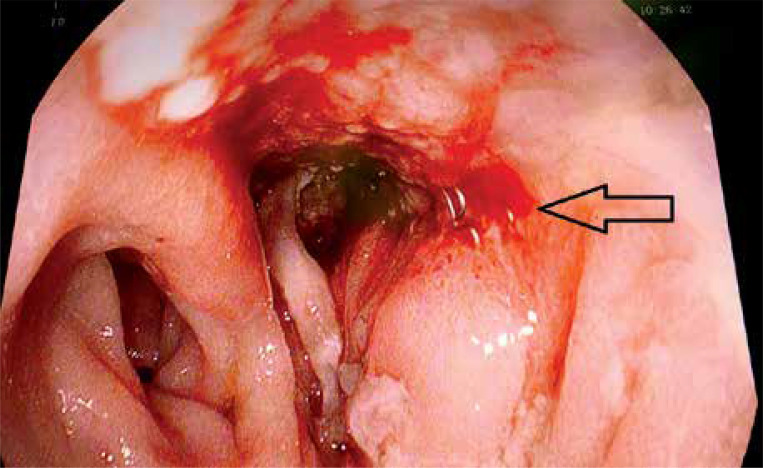
Material and methods: A group of 19 patients treated in the period 2015-2023 with postoperative upper GI tract leakage was enrolled for endoscopic treatment. The indication for the therapy was anastomotic dehiscence not exceeding half of the circumference and the absence of severe septic complications. All patients were managed using endoscopic vacuum therapy (EVT) or a self-expanding stent while persistent fistulas were additionally treated with alternative methods.
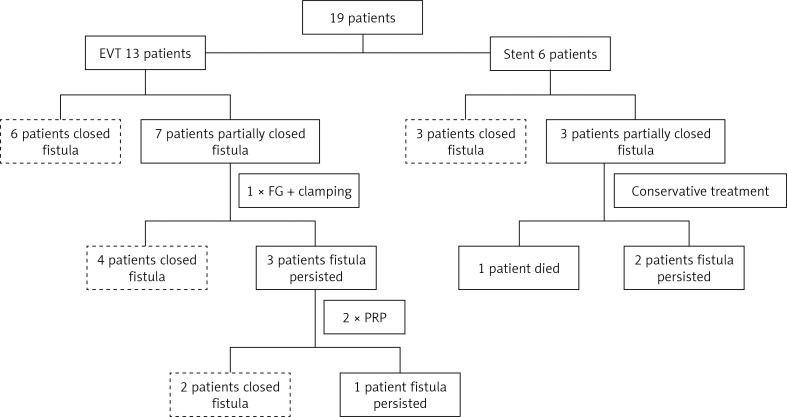
Results: The EVT was successfully implemented in 13 cases, but 7 patients required alternative methods to achieve definitive healing. Self-expanding stent placement was performed in 6 patients; however, in 3 cases a periprosthetic leakage occurred. In this group, 2 patients had the stent removed and the third one died due to septic complications. Post-treatment stenosis was identified in 5 patients after EVT that required balloon dilation with acceptable resolution in all cases.
Conclusions: Early detected anastomotic dehiscence limited to half of the circumference most effectively responded to the noninvasive treatment. Nutritional support as well as complementary endoscopic solutions such as tissue adhesives, growth stimulants and hemostatic clips increase the percentage of complete healing.
Keywords: anastomotic dehiscence; endoscopic stent implementation; endoscopic vacuum therapy; noninvasive leak treatment.
Copyright: © 2023 Fundacja Videochirurgii.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Burgos AM, Braghetto I, Csendes A, et al. Gastric leak after laparoscopic-sleeve gastrectomy for obesity. Obes Surg 2009; 19: 1672-7. - PubMed
-
- Campanile FC, Boru CE, Rizzello M, et al. Acute complications after laparoscopic bariatric procedures: update for the general surgeon. Langenbecks Arch Surg 2013; 398: 669-86. - PubMed
-
- Csendes A, Burdiles P, Burgos AM, et al. Conservative management of anastomotic leaks after 557 open gastric bypasses. Obes Surg 2005; 15: 1252-6. - PubMed
LinkOut - more resources
Full Text Sources