

Impact of three-dimensional reconstruction visualization technology on short-term and long-term outcomes after hepatectomy in patients with hepatocellular carcinoma: a propensity-score-matched and inverse probability of treatment-weighted multicenter study
- PMID: 38241321
- PMCID: PMC10942183
- DOI: 10.1097/JS9.0000000000001047
Impact of three-dimensional reconstruction visualization technology on short-term and long-term outcomes after hepatectomy in patients with hepatocellular carcinoma: a propensity-score-matched and inverse probability of treatment-weighted multicenter study
Abstract
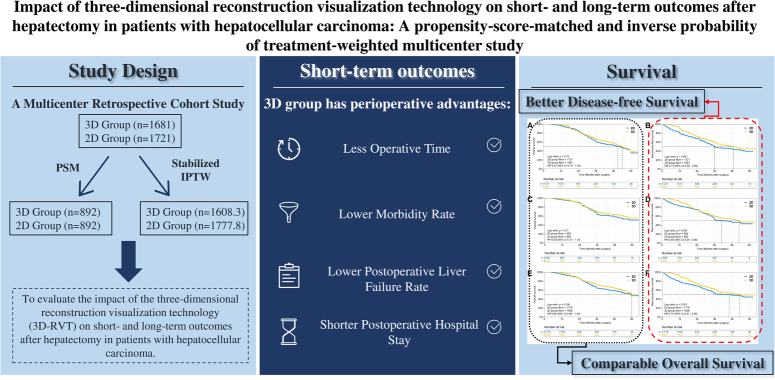
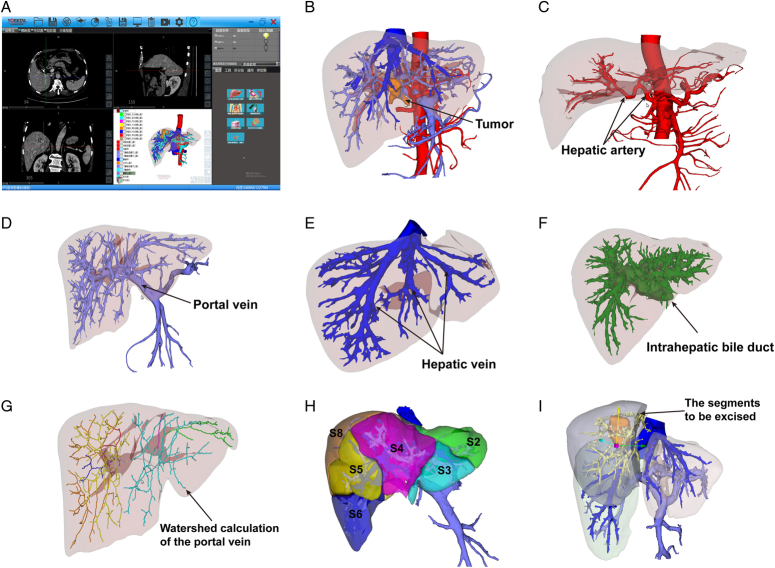
Background: Three-dimensional reconstruction visualization technology (3D-RVT) is an important tool in the preoperative assessment of patients undergoing liver resection. However, it is not clear whether this technique can improve short-term and long-term outcomes in patients with hepatocellular carcinoma (HCC) compared with two-dimensional (2D) imaging.
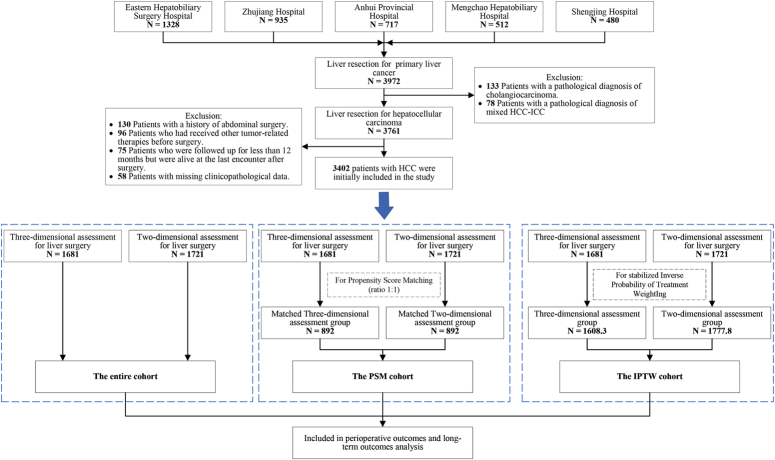
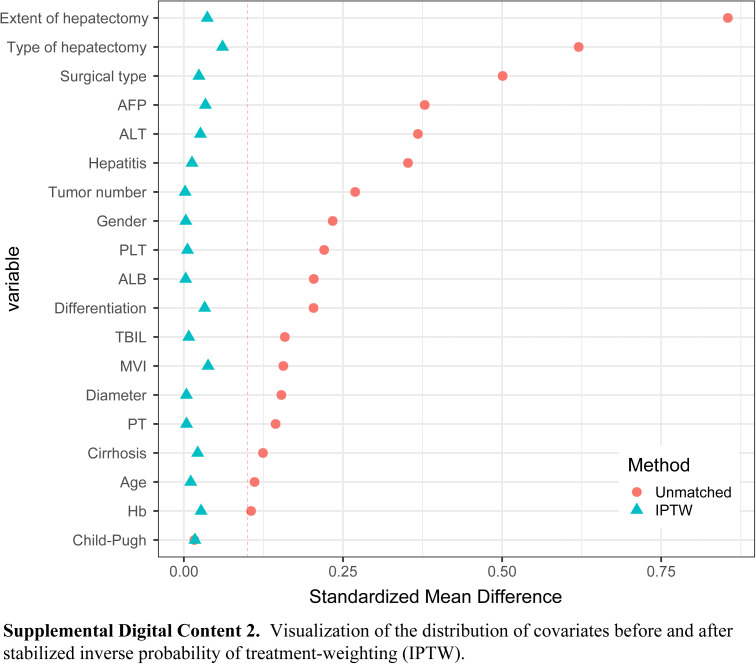
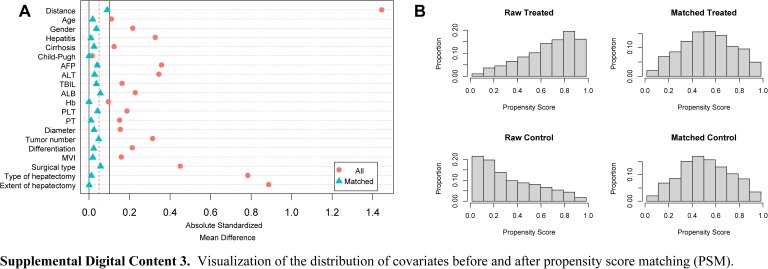
Method: A total of 3402 patients from five centers were consecutively enrolled from January 2016 to December 2020, and grouped based on the use of 3D-RVT or 2D imaging for preoperative assessment. Baseline characteristics were balanced using propensity score matching (PSM, 1:1) and stabilized inverse probability of treatment-weighting (IPTW) to reduce potential selection bias. The perioperative outcomes, long-term overall survival (OS), and recurrence-free survival (RFS) were compared between the two groups. Cox-regression analysis was used to identify the risk factors associated with RFS.
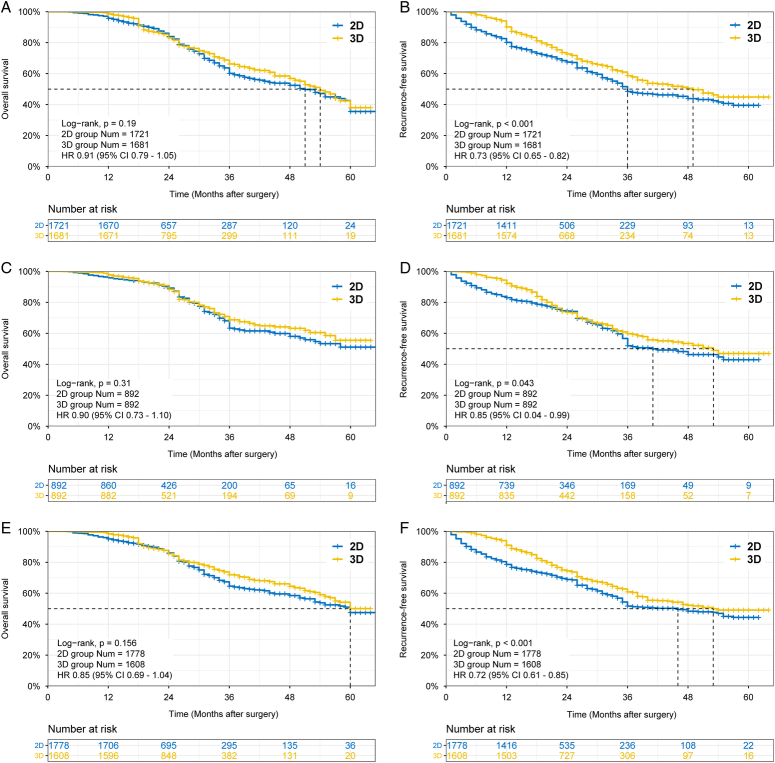
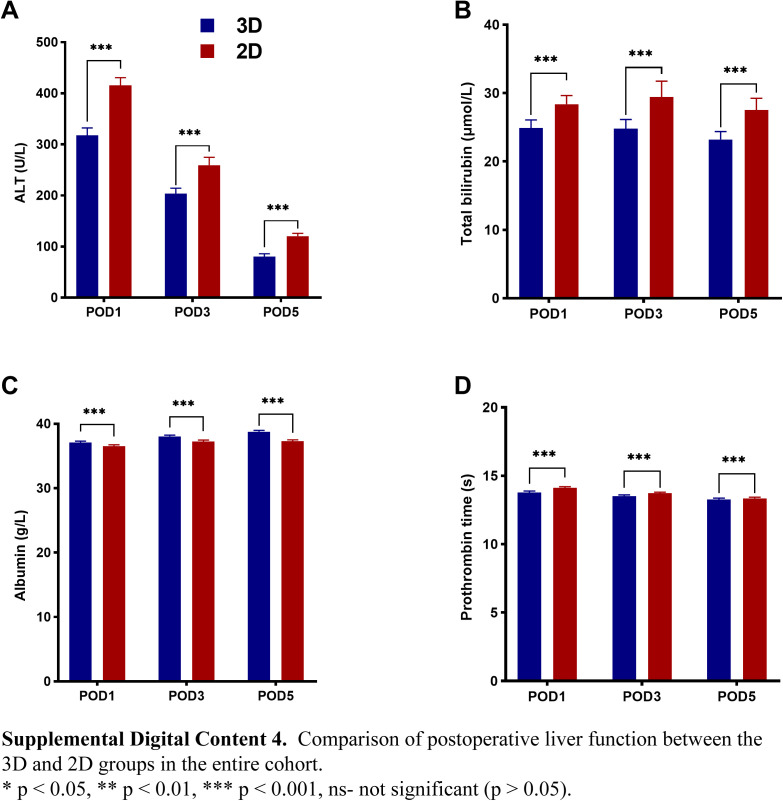
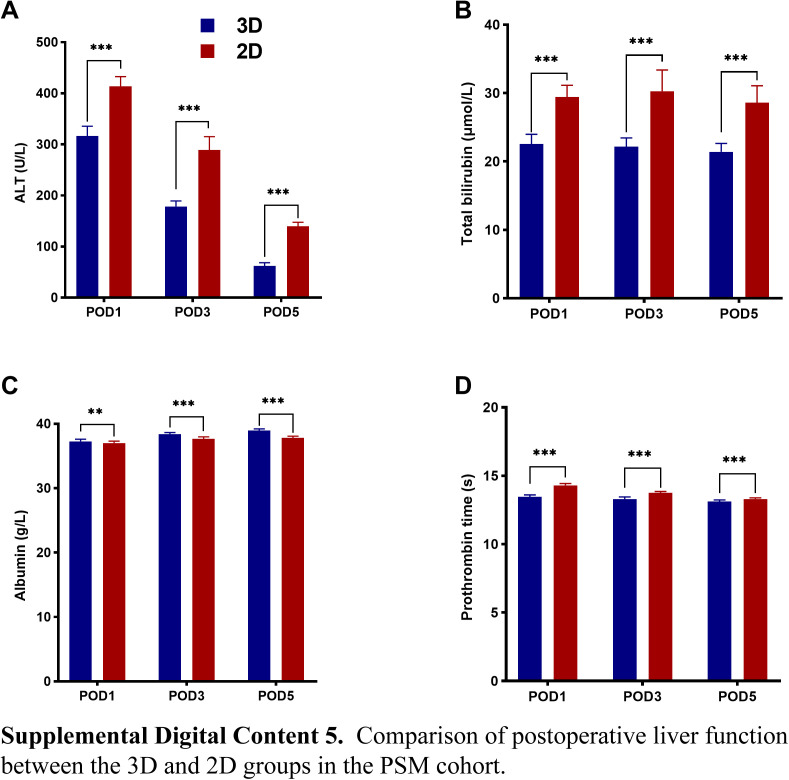
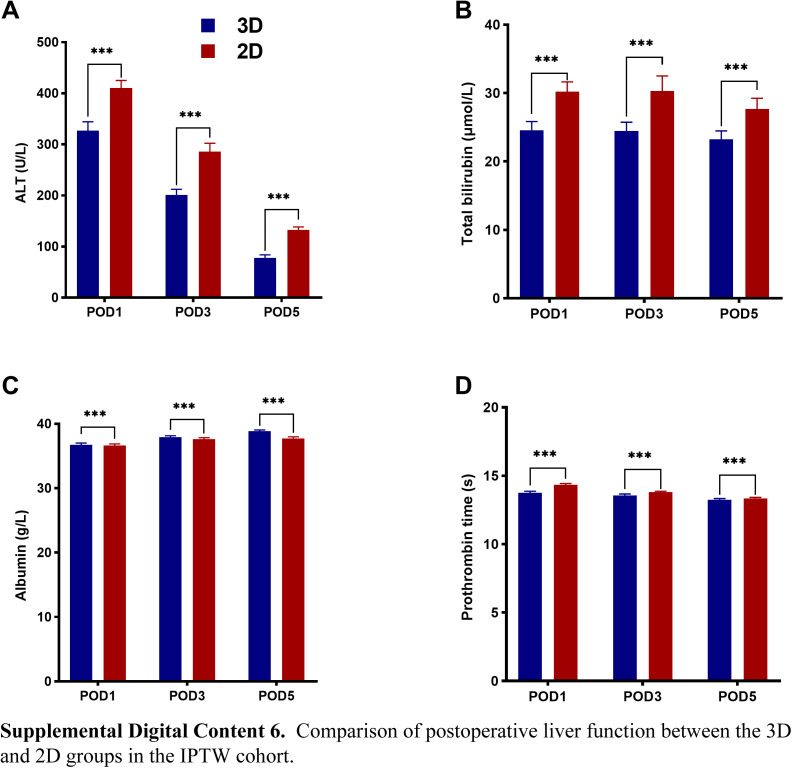
Results: A total of 1681 patients underwent 3D-RVT assessment before hepatectomy (3D group), while 1721 patients used 2D assessment (2D group). The PSM cohort included 892 patient pairs. In the IPTW cohort, there were 1608.3 patients in the 3D group and 1777.9 patients in the 2D group. In both cohorts, the 3D group had shorter operation times, lower morbidity and liver failure rates, as well as shorter postoperative hospital stays. The 3D group had more margins ≥10 mm and better RFS than the 2D group. The presence of tumors with a diameter ≥5 cm, intraoperative blood transfusion and multiple tumors were identified as independent risk factors for RFS, while 3D assessment and anatomical resection were independent protective factors.
Conclusion: In this multicenter study, perioperative outcomes and RFS of HCC patients following 3D-RVT assessment were significantly different from those following 2D imaging assessment. Thus, 3D-RVT may be a feasible alternative assessment method before hepatectomy for these patients.
Trial registration: ClinicalTrials.gov NCT05118451.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare that there are no competing interests.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Similar articles
-
Indocyanine green fluorescence imaging (ICG-FI) in difficult laparoscopic hepatectomy for hepatocellular carcinoma: a retrospective propensity score-matched analysis.Surg Endosc. 2025 May;39(5):3400-3411. doi: 10.1007/s00464-025-11707-3. Epub 2025 Apr 11. Surg Endosc. 2025. PMID: 40216627 Free PMC article.
-
[The application value of two-dimensional image technology and three-dimensional visualization technology in hepatocellular carcinoma treated by associating liver partition and portal vein ligation for staged hepatectomy: a preliminary study].Zhonghua Wai Ke Za Zhi. 2016 Sep 1;54(9):686-91. doi: 10.3760/cma.j.issn.0529-5815.2016.09.008. Zhonghua Wai Ke Za Zhi. 2016. PMID: 27587212 Chinese.
-
Perioperative and long-term survival outcomes of laparoscopic versus laparotomic hepatectomy for BCLC stages 0-A hepatocellular carcinoma patients associated with or without microvascular invasion: a multicenter, propensity score matching analysis.Hepatol Int. 2022 Aug;16(4):892-905. doi: 10.1007/s12072-022-10353-4. Epub 2022 Jun 15. Hepatol Int. 2022. PMID: 35704267
-
Association of Adjuvant Radiation Therapy With Long-Term Overall and Recurrence-Free Survival After Hepatectomy for Hepatocellular Carcinoma: A Multicenter Propensity-Matched Study.Int J Radiat Oncol Biol Phys. 2022 Oct 1;114(2):238-249. doi: 10.1016/j.ijrobp.2022.05.020. Epub 2022 May 26. Int J Radiat Oncol Biol Phys. 2022. PMID: 35643251
-
A meta-analysis of the three-dimensional reconstruction visualization technology for hepatectomy.Asian J Surg. 2023 Feb;46(2):669-676. doi: 10.1016/j.asjsur.2022.07.006. Epub 2022 Jul 14. Asian J Surg. 2023. PMID: 35843827 Review.
Cited by
-
Impact of three-dimensional reconstruction visualization technology on short-term and long-term outcomes after hepatectomy in patients with hepatocellular carcinoma: a propensity-score-matched and inverse probability of treatment-weighted multicenter study: Erratum.Int J Surg. 2024 May 1;110(5):3137. doi: 10.1097/JS9.0000000000001623. Int J Surg. 2024. PMID: 38748503 Free PMC article. No abstract available.
-
Sorafenib with or without co-interventions for hepatocellular carcinoma.Cochrane Database Syst Rev. 2025 Jun 26;6(6):CD015851. doi: 10.1002/14651858.CD015851. Cochrane Database Syst Rev. 2025. PMID: 40568833 Free PMC article. Review.
-
ASO Author Reflections: Real-Time Bile-Duct-Obstructed Area Fluorescence Imaging Guided Laparoscopic Hepatectomy: A Novel Navigation Strategy for Localized Intrahepatic Biliary Obstruction.Ann Surg Oncol. 2024 Dec;31(13):9237-9239. doi: 10.1245/s10434-024-16138-3. Epub 2024 Sep 2. Ann Surg Oncol. 2024. PMID: 39223378 No abstract available.
-
Laparoscopic left hemihepatectomy using augmented reality navigation plus ICG fluorescence imaging for hepatolithiasis: a retrospective single-arm cohort study (with video).Surg Endosc. 2024 Jul;38(7):4048-4056. doi: 10.1007/s00464-024-10922-8. Epub 2024 May 28. Surg Endosc. 2024. PMID: 38806956
-
Long-Term Outcomes of Laparoscopic Anatomical versus Non-Anatomical Liver Resection for Hepatocellular Carcinoma.J Hepatocell Carcinoma. 2024 Dec 5;11:2413-2425. doi: 10.2147/JHC.S483014. eCollection 2024. J Hepatocell Carcinoma. 2024. PMID: 39659771 Free PMC article.
References
-
- Vogel A, Meyer T, Sapisochin G, et al. . Hepatocellular carcinoma. Lancet 2022;400:1345–1362. - PubMed
-
- Vibert E, Schwartz M, Olthoff KM. Advances in resection and transplantation for hepatocellular carcinoma. J Hepatol 2020;72:262–276. - PubMed
-
- Yang T, Lin S, Xie Q, et al. . Impact of 3D printing technology on the comprehension of surgical liver anatomy. Surg Endosc 2019;33:411–417. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
