

Recent advances in the management of immune thrombocytopenic purpura (ITP): A comprehensive review
- PMID: 38241567
- PMCID: PMC10798712
- DOI: 10.1097/MD.0000000000036936
Recent advances in the management of immune thrombocytopenic purpura (ITP): A comprehensive review
Abstract
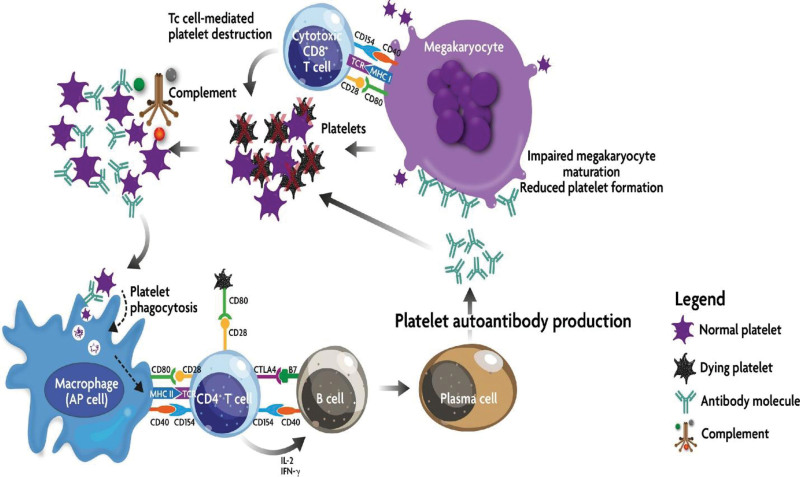
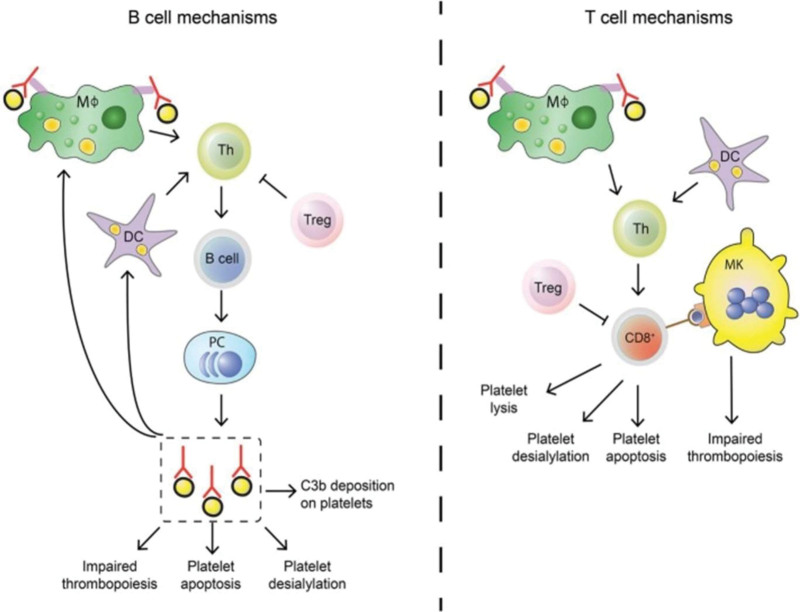
Autoimmune disorders place a substantial burden on the healthcare system all over the world affecting almost 3% to 8% of the population. Immune thrombocytopenic purpura (ITP), also known as idiopathic thrombocytopenic purpura, is a blood disorder in which the body immune system destroys platelets, leading to low platelet counts in the blood (peripheral blood platelet count < 150 × 109/L). Although the pathophysiology of ITP is not fully understood, it is believed to result from a complex interplay between hereditary and environmental variables. Certain factors, such as a low platelet count, history of bleeding, and certain comorbidities can increase the risk of severe bleeding in patients with ITP. Corticosteroids, intravenous immunoglobulin (IVIG), immunosuppressants, rituximab, and thrombopoietin receptor agonists (TPO-RAs) are some of the advanced treatments for ITP. Although these therapies may be successful, they also carry the risk of negative effects. Recently, significant advancements have been made in the understanding and treatment of ITP. There is still much to learn about the disease, and new, more effective treatments are needed. This comprehensive review offers a comprehensive assessment of recent advancements in ITP management, with a focus on active research projects, novel therapeutic targets, new treatment modalities, and areas of uncertainty and unmet needs. According to research, it is crucial to develop individualized treatment plans for ITP patients based on their age, platelet count, risk of bleeding, and comorbidities. The article also looks at how future developments in gene editing, bispecific antibody therapies, and cellular therapy may completely change the treatment of ITP.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
First-line therapies for immune thrombocytopenic purpura: re-evaluating the need to treat.Eur J Haematol Suppl. 2008 Feb;(69):19-26. doi: 10.1111/j.1600-0609.2007.01000.x. Eur J Haematol Suppl. 2008. PMID: 18211569 Review.
-
Current approaches for the diagnosis and management of immune thrombocytopenia.Eur J Intern Med. 2023 Feb;108:18-24. doi: 10.1016/j.ejim.2022.11.022. Epub 2022 Nov 21. Eur J Intern Med. 2023. PMID: 36424271 Review.
-
Thrombopoietin receptor agonists for preparing adult patients with immune thrombocytopenia to splenectomy: results of a retrospective, observational GIMEMA study.Am J Hematol. 2016 May;91(5):E293-5. doi: 10.1002/ajh.24341. Epub 2016 Apr 4. Am J Hematol. 2016. PMID: 26910388
-
Cost-effectiveness of adding rituximab to splenectomy and romiplostim for treating steroid-resistant idiopathic thrombocytopenic purpura in adults.BMC Health Serv Res. 2015 Jan 22;15:2. doi: 10.1186/s12913-015-0681-y. BMC Health Serv Res. 2015. PMID: 25609557 Free PMC article.
-
[Diagnostic approach and treatment of immune thrombocytopenia in adults].Acta Med Croatica. 2013 Mar;67(1):3-11. Acta Med Croatica. 2013. PMID: 24279250 Review. Croatian.
Cited by
-
Navigating Primary Immune Thrombocytopenia During Pregnancy With Management Strategies and Considerations: A Comprehensive Review.Cureus. 2024 Aug 21;16(8):e67449. doi: 10.7759/cureus.67449. eCollection 2024 Aug. Cureus. 2024. PMID: 39314573 Free PMC article. Review.
-
Detection of Thrombosis Using Soluble C-Type Lectin-like Receptor-2 with D-Dimer Level and Platelet Count.J Clin Med. 2024 Oct 8;13(19):5980. doi: 10.3390/jcm13195980. J Clin Med. 2024. PMID: 39408040 Free PMC article.
-
The gut-immune axis in primary immune thrombocytopenia (ITP): a paradigm shifts in treatment approaches.Front Immunol. 2025 Jun 12;16:1595977. doi: 10.3389/fimmu.2025.1595977. eCollection 2025. Front Immunol. 2025. PMID: 40574831 Free PMC article. Review.
-
When Platelets Fail: A Case of Active Gastrointestinal Bleeding in Immune Thrombocytopenia.Cureus. 2025 Jun 13;17(6):e85927. doi: 10.7759/cureus.85927. eCollection 2025 Jun. Cureus. 2025. PMID: 40656329 Free PMC article.
-
On the horizon: upcoming new agents for the management of ITP.Hematology Am Soc Hematol Educ Program. 2024 Dec 6;2024(1):692-699. doi: 10.1182/hematology.2024000596. Hematology Am Soc Hematol Educ Program. 2024. PMID: 39644072 Free PMC article. Review.
References
-
- Blanchette M, Freedman J. The history of idiopathic thrombocytopenic purpura (ITP). Transfus Sci. 1998;19:231–6. - PubMed
-
- British Committee for Standards in Haematology General Haematology Task F. Guidelines for the investigation and management of idiopathic thrombocytopenic purpura in adults, children and in pregnancy. Br J Haematol. 2003;120:574–96. - PubMed
-
- Piel-Julian ML, Mahevas M, Germain J, et al. . Risk factors for bleeding, including platelet count threshold, in newly diagnosed immune thrombocytopenia adults. J Thromb Haemost. 2018;16:1830–42. - PubMed
-
- Adelborg K, Kristensen NR, Norgaard M, et al. . Cardiovascular and bleeding outcomes in a population-based cohort of patients with chronic immune thrombocytopenia. J Thromb Haemost. 2019;17:912–24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
