

Hypoxia-Directed Treatment of Human Papillomavirus-Related Oropharyngeal Carcinoma
- PMID: 38241600
- PMCID: PMC10927322
- DOI: 10.1200/JCO.23.01308
Hypoxia-Directed Treatment of Human Papillomavirus-Related Oropharyngeal Carcinoma
Abstract
Purpose: Standard curative-intent chemoradiotherapy for human papillomavirus (HPV)-related oropharyngeal carcinoma results in significant toxicity. Since hypoxic tumors are radioresistant, we posited that the aerobic state of a tumor could identify patients eligible for de-escalation of chemoradiotherapy while maintaining treatment efficacy.
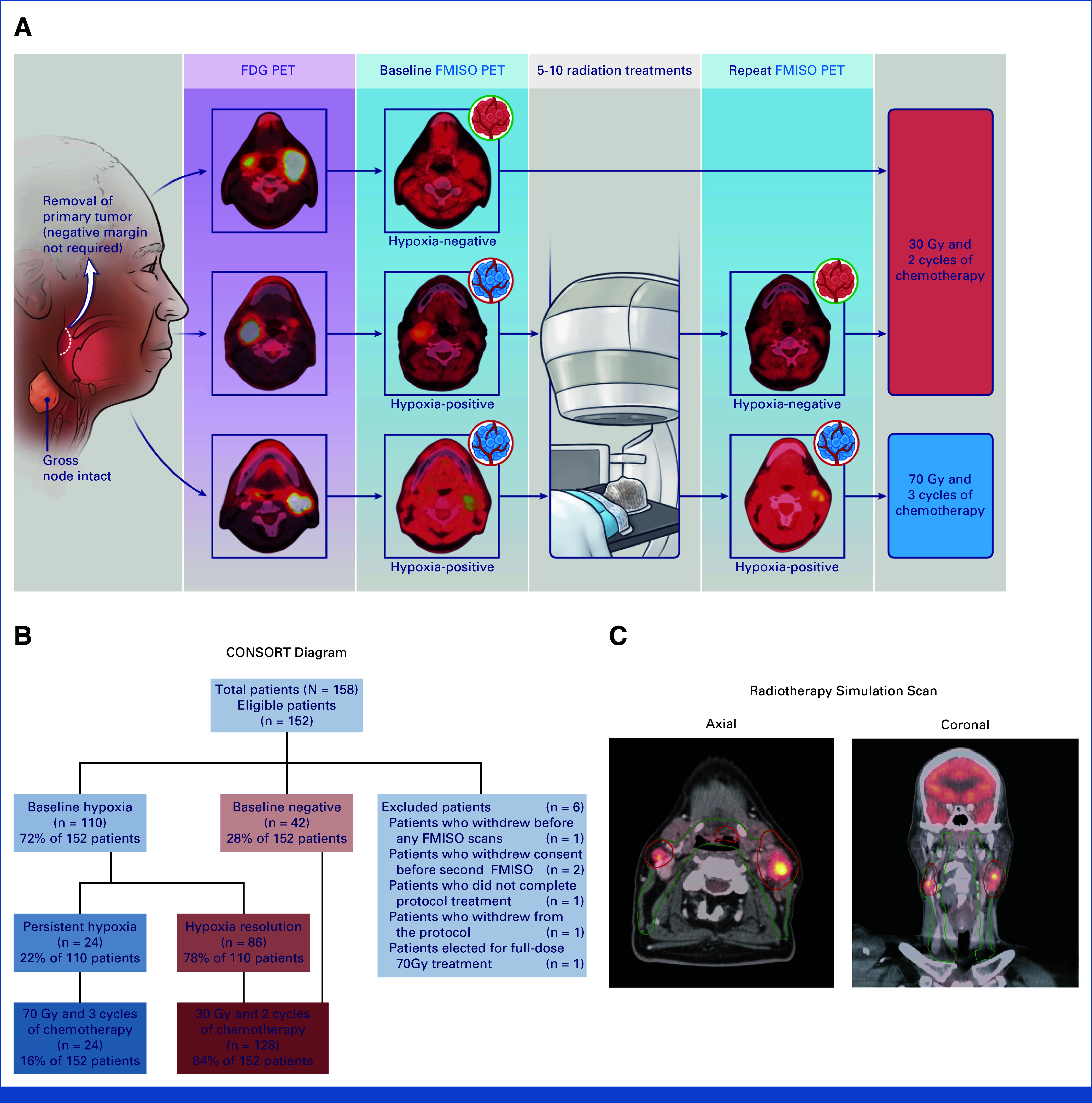
Methods: We enrolled patients with HPV-related oropharyngeal carcinoma to receive de-escalated definitive chemoradiotherapy in a phase II study (ClinicalTrials.gov identifier: NCT03323463). Patients first underwent surgical removal of disease at their primary site, but not of gross disease in the neck. A baseline 18F-fluoromisonidazole positron emission tomography scan was used to measure tumor hypoxia and was repeated 1-2 weeks intratreatment. Patients with nonhypoxic tumors received 30 Gy (3 weeks) with chemotherapy, whereas those with hypoxic tumors received standard chemoradiotherapy to 70 Gy (7 weeks). The primary objective was achieving a 2-year locoregional control (LRC) of 95% with a 7% noninferiority margin.
Results: One hundred fifty-eight patients with T0-2/N1-N2c were enrolled, of which 152 patients were eligible for analyses. Of these, 128 patients met criteria for 30 Gy and 24 patients received 70 Gy. The 2-year LRC was 94.7% (95% CI, 89.8 to 97.7), meeting our primary objective. With a median follow-up time of 38.3 (range, 22.1-58.4) months, the 2-year progression-free survival (PFS) and overall survival (OS) rates were 94% and 100%, respectively, for the 30-Gy cohort. The 70-Gy cohort had similar 2-year PFS and OS rates at 96% and 96%, respectively. Acute grade 3-4 adverse events were more common in 70 Gy versus 30 Gy (58.3% v 32%; P = .02). Late grade 3-4 adverse events only occurred in the 70-Gy cohort, in which 4.5% complained of late dysphagia.
Conclusion: Tumor hypoxia is a promising approach to direct dosing of curative-intent chemoradiotherapy for HPV-related carcinomas with preserved efficacy and substantially reduced toxicity that requires further investigation.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures


References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
