

Patterns of comorbidities differentially affect long-term functional evolution and disease activity in patients with 'difficult to treat' rheumatoid arthritis
- PMID: 38242549
- PMCID: PMC10806522
- DOI: 10.1136/rmdopen-2023-003808
Patterns of comorbidities differentially affect long-term functional evolution and disease activity in patients with 'difficult to treat' rheumatoid arthritis
Abstract
Background: Characterisation of the long-term outcome of patients with 'difficult to treat' (D2T) rheumatoid arthritis and factors contributing to its evolution are unknown. Herein, we explored the heterogeneity and contributing factors of D2T long-term outcome.
Methods: Patients included from a prospective single centre cohort study. The EULAR definition of D2T was applied. Longitudinal clustering of functional status (modified Health Assessment Questionnaire (mHAQ)) and disease activity (Disease Activity Score-28 (DAS28)) were assessed using latent-class trajectory analysis. Multiple linear mixed models were used to examine the impact of comorbidities and their clusters on the long-term outcome.
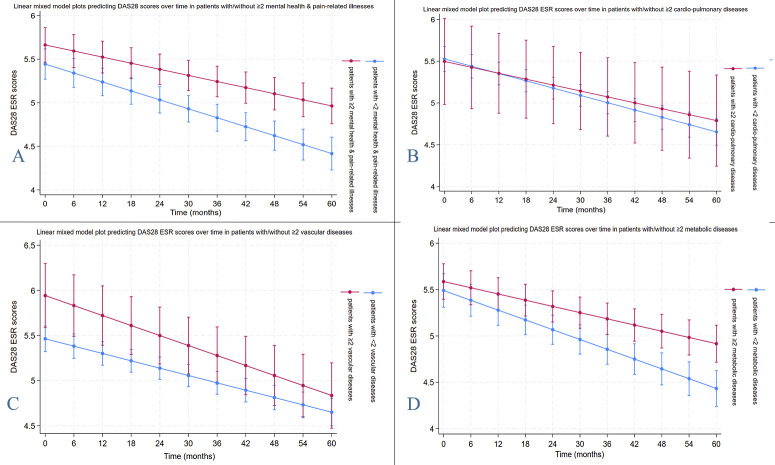
Results: 251 out of 1264 patients (19.9%) were identified as D2T. Younger age, fibromyalgia, osteoarthritis, DAS28-erythrocyte sedimentation rate (ESR) at first biological or targeted synthetic disease-modifying antirheumatic drug (b/ts-DMARD) initiation and failure to reduce DAS28-ESR scores within the first 6 months of b/ts-DMARD therapy were significant predictors of patients becoming D2T. Long-term follow-up (total of 5872 person-years) revealed four groups of functional status evolution: 18.2% had stable, mildly compromised mHAQ (mean 0.41), 39.9% had gradual improvement (1.21-0.87) and two groups had either slow deterioration or stable significant functional impairment (HAQ>1). Similarly, four distinct groups of disease activity evolution were identified. Among the different clusters of comorbidities assessed, presence of 'mental-health and pain-related illnesses' or 'metabolic diseases' had significant contribution to mHAQ worsening (p<0.0001 for both) and DAS28 evolution (p<0.0001 and p=0.018, respectively).
Conclusion: D2T patients represent a heterogeneous group in terms of long-term disease course. Mental-health/pain-related illnesses as well as metabolic diseases contribute to long-term adverse outcomes and should be targeted in order to optimise the prognosis of this subset of rheumatoid arthritis.
Keywords: Outcome Assessment, Health Care; Patient Reported Outcome Measures; Rheumatoid Arthritis.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous