

Evaluation of potential biomarkers for lenvatinib plus pembrolizumab among patients with advanced endometrial cancer: results from Study 111/KEYNOTE-146
- PMID: 38242717
- PMCID: PMC10806562
- DOI: 10.1136/jitc-2023-007929
Evaluation of potential biomarkers for lenvatinib plus pembrolizumab among patients with advanced endometrial cancer: results from Study 111/KEYNOTE-146
Abstract
Background: Lenvatinib plus pembrolizumab demonstrated clinically meaningful benefit in patients with previously treated advanced endometrial carcinoma in Study 111/KEYNOTE-146 (NCT02501096). In these exploratory analyses from this study, we evaluated the associations between clinical outcomes and gene expression signature scores and descriptively summarized response in biomarker subpopulations defined by tumor mutational burden (TMB) and DNA variants for individual genes of interest.
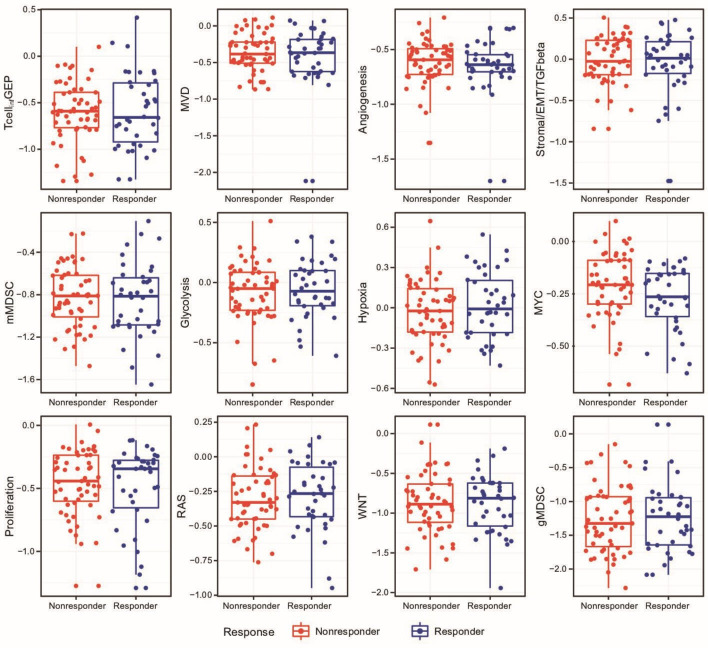
Methods: Patients with histologically confirmed metastatic endometrial carcinoma received oral lenvatinib 20 mg once daily plus intravenous pembrolizumab 200 mg every 3 weeks for 35 cycles. Archived formalin-fixed paraffin-embedded tissue was obtained from all patients. T-cell-inflamed gene expression profile (TcellinfGEP) and 11 other gene signatures were evaluated by RNA sequencing. TMB, hotspot mutations in PIK3CA (oncogene), and deleterious mutations in PTEN and TP53 (tumor suppressor genes) were evaluated by whole-exome sequencing (WES).
Results: 93 and 79 patients were included in the RNA-sequencing-evaluable and WES-evaluable populations, respectively. No statistically significant associations were observed between any of the RNA-sequencing signature scores and objective response rate or progression-free survival. Area under the receiver operating characteristic curve values for response ranged from 0.39 to 0.54; all 95% CIs included 0.50. Responses were seen regardless of TMB (≥175 or <175 mutations/exome) and mutation status. There were no correlations between TcellinfGEP and TMB, TcellinfGEP and microvessel density (MVD), or MVD and TMB.
Conclusions: This analysis demonstrated efficacy for lenvatinib plus pembrolizumab regardless of biomarker status. Results from this study do not support clinical utility of the evaluated biomarkers. Further investigation of biomarkers for this regimen is warranted.
Trial registration number: NCT02501096.
Keywords: Immunotherapy; Tumor Biomarkers.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: VM is supported in part by the NIH/NCI Cancer Center Support Grant P30 CA008748. Study support (all funding to institution)/unpaid consultancy/advisory board membership from AstraZeneca, Clovis, Duality, Eisai, Faeth, Genentech, GSK, Immunocore, iTEOS, Kartos, Karyopharm, Moreo, Morphosys, MSD, Novartis, Takeda, and Zymeworks. MHT received honoraria for consulting/advisory board participation from Bristol-Myers Squibb, Eisai Inc, Novartis, Merck & Co., Inc., Pfizer, Bayer, Sanofi/Genzyme, Regeneron, LOXO Oncology, Blueprint Medicines, Immune-onc, Exelixis, and Cascade Prodrug. MHT received honoraria for participation in speakers' bureaus from Bristol-Myers Squibb, Eisai Inc, Blueprint Medicines, and Merck & Co., Inc. Research funding to Dr Taylor’s institution was provided by Bristol-Myers Squibb, Eisai, Merck & Co., Inc., Pfizer, Immune-Onc, and Simcha. CA: Clinical trial funding (to institution): AbbVie, Artios Pharma, AstraZeneca, Clovis, and Genentech/Roche; Advisory board (fees): Merck; Advisory board (no fees): Blueprint Medicine; Data Monitoring Committee: AstraZeneca; Leadership role: GOG Foundation, Board of Directors (travel cost reimbursement for attending meetings) and NRG Oncology, Board of Directors (unpaid). CA is supported in part by the NIH/NCI Cancer Center Support Grant P30 CA008748. ALC: Honoraria: Amgen; Expert Testimony: Department of Justice. MSB: Consulting/advisory board member (honoraria paid to me): Eisai Inc, Exelixis, Loxo Oncology, Eli Lilly, and Bayer Pharmaceuticals. CDS: Nothing to disclose. ZAC, AL, RC, PJ, and RO: Employees of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and stockholders in Merck & Co., Inc., Rahway, NJ, USA. LS: Employee of Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA. LD, JM, and CED: Employees of Eisai Inc., Nutley, NJ, USA. YM: Employee of Eisai Co. Ltd., Tsukuba, Japan, and a stockholder in Eisai Co., Ltd. MJM: Nothing to disclose.
Figures



References
-
- Howlader N, Noone AM, Krapcho M, et al. . SEER cancer statistics review, 1975-2017. Available: https://seer.cancer.gov/archive/csr/1975_2017 [Accessed 27 Sep 2023].
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous