

"KAIZEN" method realizing implementation of deep-learning models for COVID-19 CT diagnosis in real world hospitals
- PMID: 38243054
- PMCID: PMC10799049
- DOI: 10.1038/s41598-024-52135-y
"KAIZEN" method realizing implementation of deep-learning models for COVID-19 CT diagnosis in real world hospitals
Abstract
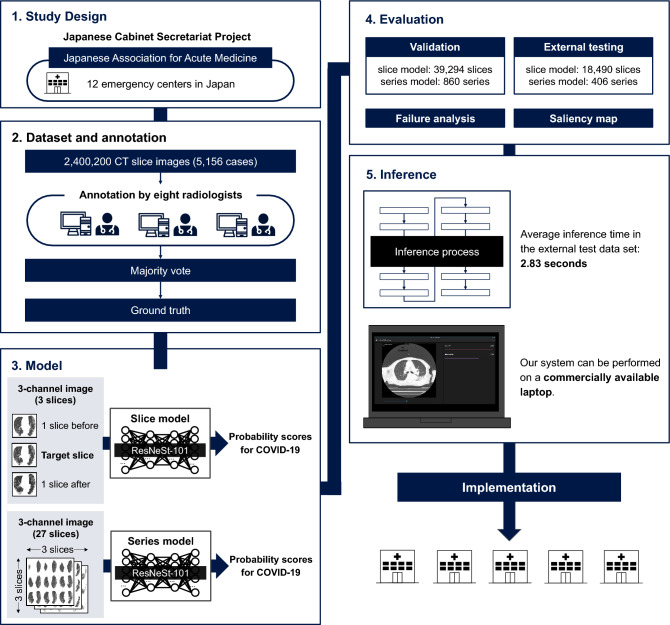
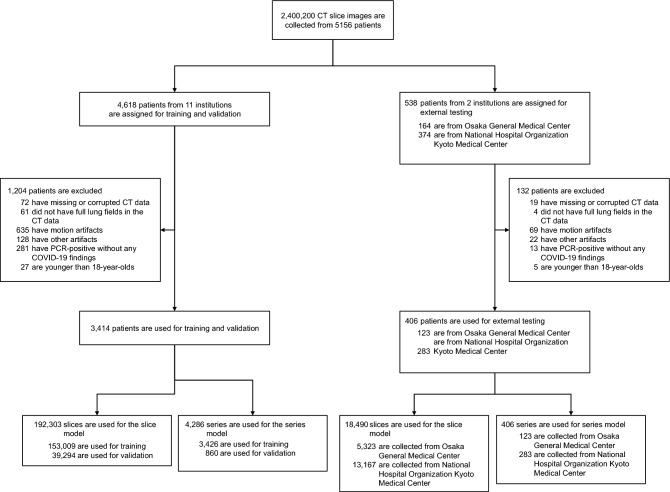
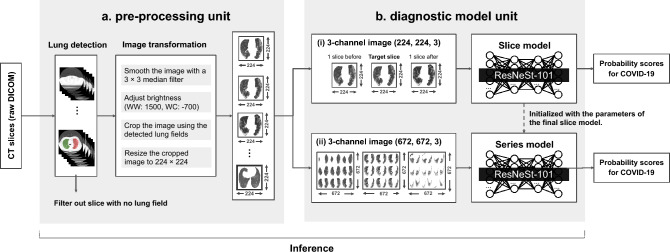
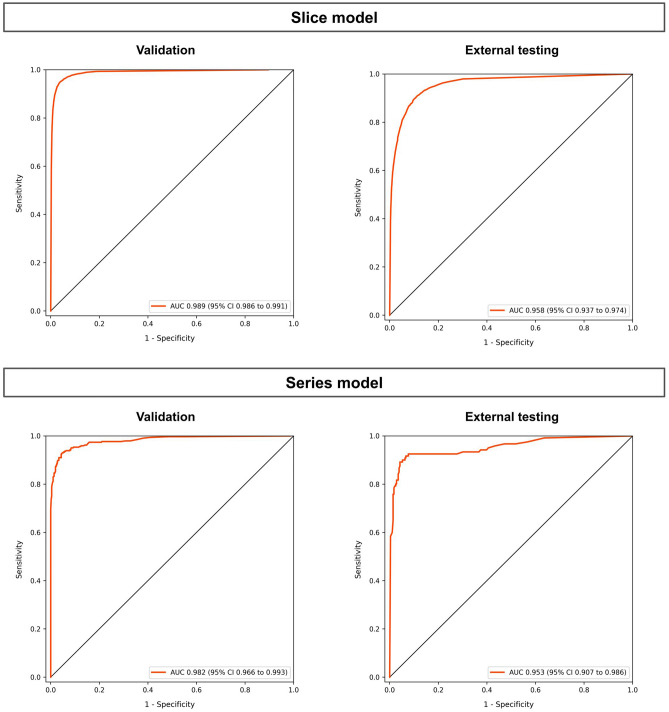
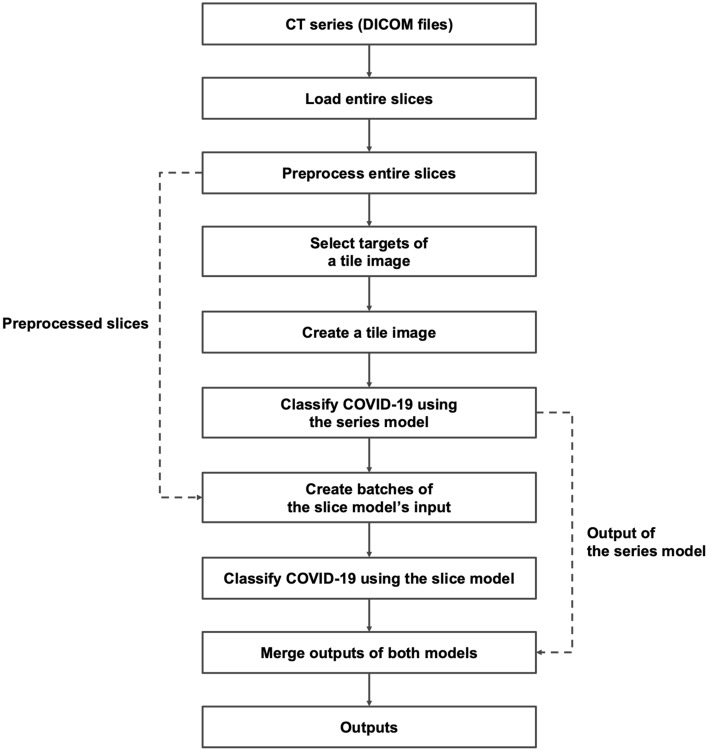
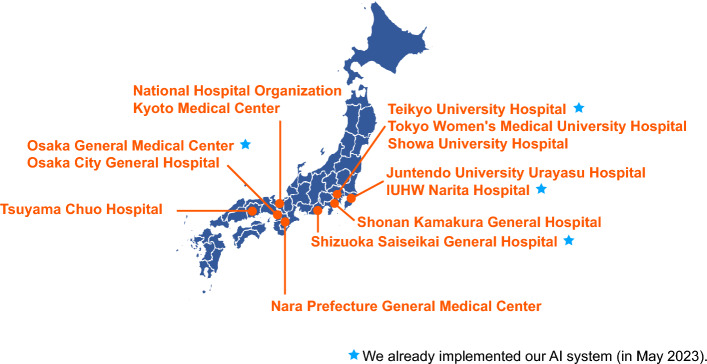
Numerous COVID-19 diagnostic imaging Artificial Intelligence (AI) studies exist. However, none of their models were of potential clinical use, primarily owing to methodological defects and the lack of implementation considerations for inference. In this study, all development processes of the deep-learning models are performed based on strict criteria of the "KAIZEN checklist", which is proposed based on previous AI development guidelines to overcome the deficiencies mentioned above. We develop and evaluate two binary-classification deep-learning models to triage COVID-19: a slice model examining a Computed Tomography (CT) slice to find COVID-19 lesions; a series model examining a series of CT images to find an infected patient. We collected 2,400,200 CT slices from twelve emergency centers in Japan. Area Under Curve (AUC) and accuracy were calculated for classification performance. The inference time of the system that includes these two models were measured. For validation data, the slice and series models recognized COVID-19 with AUCs and accuracies of 0.989 and 0.982, 95.9% and 93.0% respectively. For test data, the models' AUCs and accuracies were 0.958 and 0.953, 90.0% and 91.4% respectively. The average inference time per case was 2.83 s. Our deep-learning system realizes accuracy and inference speed high enough for practical use. The systems have already been implemented in four hospitals and eight are under progression. We released an application software and implementation code for free in a highly usable state to allow its use in Japan and globally.
© 2024. The Author(s).
Conflict of interest statement
Naoki Okada received grants from the Japanese Cabinet Secretariat (438-2020-5E, 834-2021-4A, 847-2022-2C, 847-2022-2D). Naoki Okada and Shusuke Inoue are board members of fcuro inc. Shun Honda and Yuichiro Hirano are employees of fcuro inc. Other authors declare no competing interests.
Figures
Similar articles
-
Six artificial intelligence paradigms for tissue characterisation and classification of non-COVID-19 pneumonia against COVID-19 pneumonia in computed tomography lungs.Int J Comput Assist Radiol Surg. 2021 Mar;16(3):423-434. doi: 10.1007/s11548-021-02317-0. Epub 2021 Feb 3. Int J Comput Assist Radiol Surg. 2021. PMID: 33532975 Free PMC article.
-
From community-acquired pneumonia to COVID-19: a deep learning-based method for quantitative analysis of COVID-19 on thick-section CT scans.Eur Radiol. 2020 Dec;30(12):6828-6837. doi: 10.1007/s00330-020-07042-x. Epub 2020 Jul 18. Eur Radiol. 2020. PMID: 32683550 Free PMC article.
-
A deep learning-based application for COVID-19 diagnosis on CT: The Imaging COVID-19 AI initiative.PLoS One. 2023 May 2;18(5):e0285121. doi: 10.1371/journal.pone.0285121. eCollection 2023. PLoS One. 2023. PMID: 37130128 Free PMC article.
-
A narrative review on characterization of acute respiratory distress syndrome in COVID-19-infected lungs using artificial intelligence.Comput Biol Med. 2021 Mar;130:104210. doi: 10.1016/j.compbiomed.2021.104210. Epub 2021 Jan 18. Comput Biol Med. 2021. PMID: 33550068 Free PMC article. Review.
-
Utilisation of deep learning for COVID-19 diagnosis.Clin Radiol. 2023 Feb;78(2):150-157. doi: 10.1016/j.crad.2022.11.006. Clin Radiol. 2023. PMID: 36639173 Free PMC article. Review.
Cited by
-
AI based medical imagery diagnosis for COVID-19 disease examination and remedy.Sci Rep. 2025 Jan 10;15(1):1607. doi: 10.1038/s41598-024-84644-1. Sci Rep. 2025. PMID: 39794454 Free PMC article.
References
-
- World Health Organization. Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases: Interim guidance (2020) https://apps.who.int/iris/bitstream/handle/10665/331329/WHO-COVID-19-lab....
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
