

Evolution of radiation-induced temporal lobe injury after intensity-modulated radiation therapy in nasopharyngeal carcinoma: a large cohort retrospective study
- PMID: 38243277
- PMCID: PMC10797916
- DOI: 10.1186/s13014-024-02400-1
Evolution of radiation-induced temporal lobe injury after intensity-modulated radiation therapy in nasopharyngeal carcinoma: a large cohort retrospective study
Erratum in
-
Correction: Evolution of radiation-induced temporal lobe injury after intensity-modulated radiation therapy in nasopharyngeal carcinoma: a large cohort retrospective study.Radiat Oncol. 2024 Mar 27;19(1):41. doi: 10.1186/s13014-024-02423-8. Radiat Oncol. 2024. PMID: 38539196 Free PMC article. No abstract available.
Abstract
Background: Previous studies have demonstrated conflicting findings regarding the initial MRI patterns of radiotherapy-induced temporal lobe injury (RTLI) and the evolution of different RTLI patterns. The aim of this study was to evaluate the initial MRI pattern and evolution of RTLI in patients with nasopharyngeal carcinoma (NPC) by means of a large cohort study.
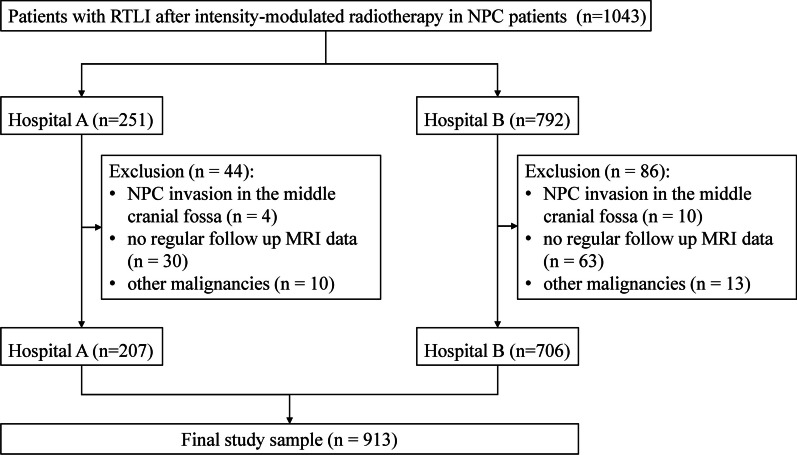
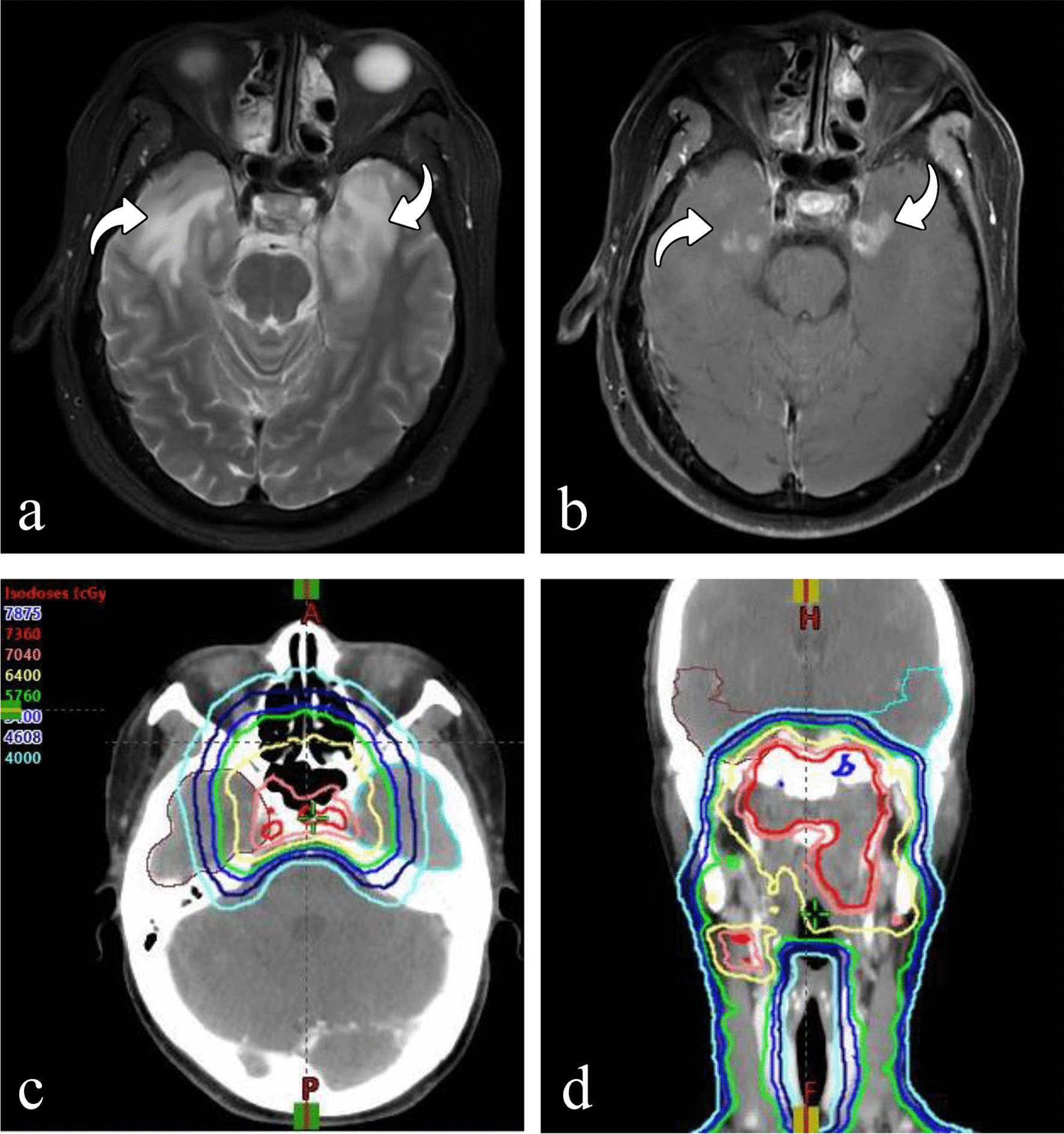
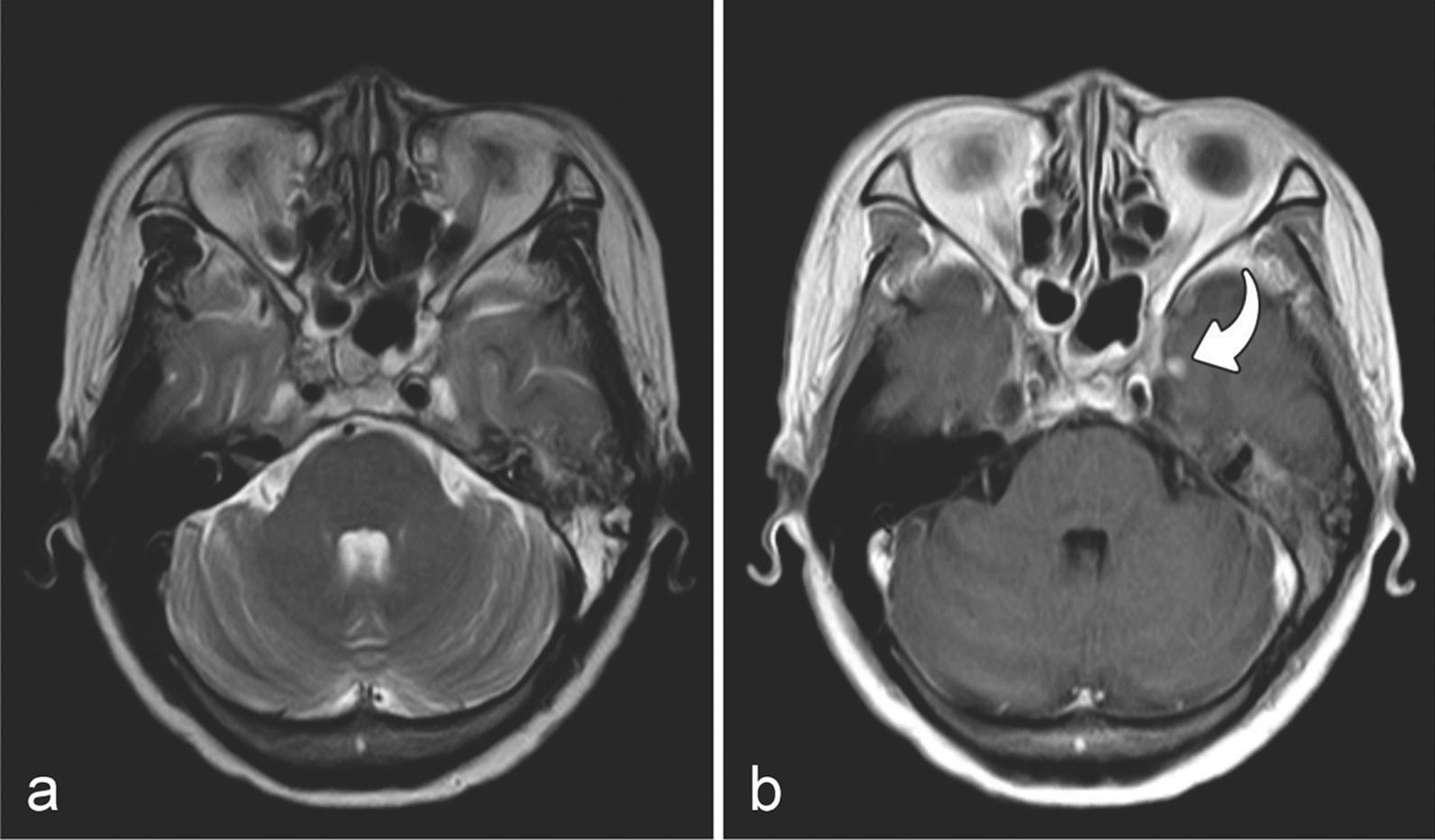
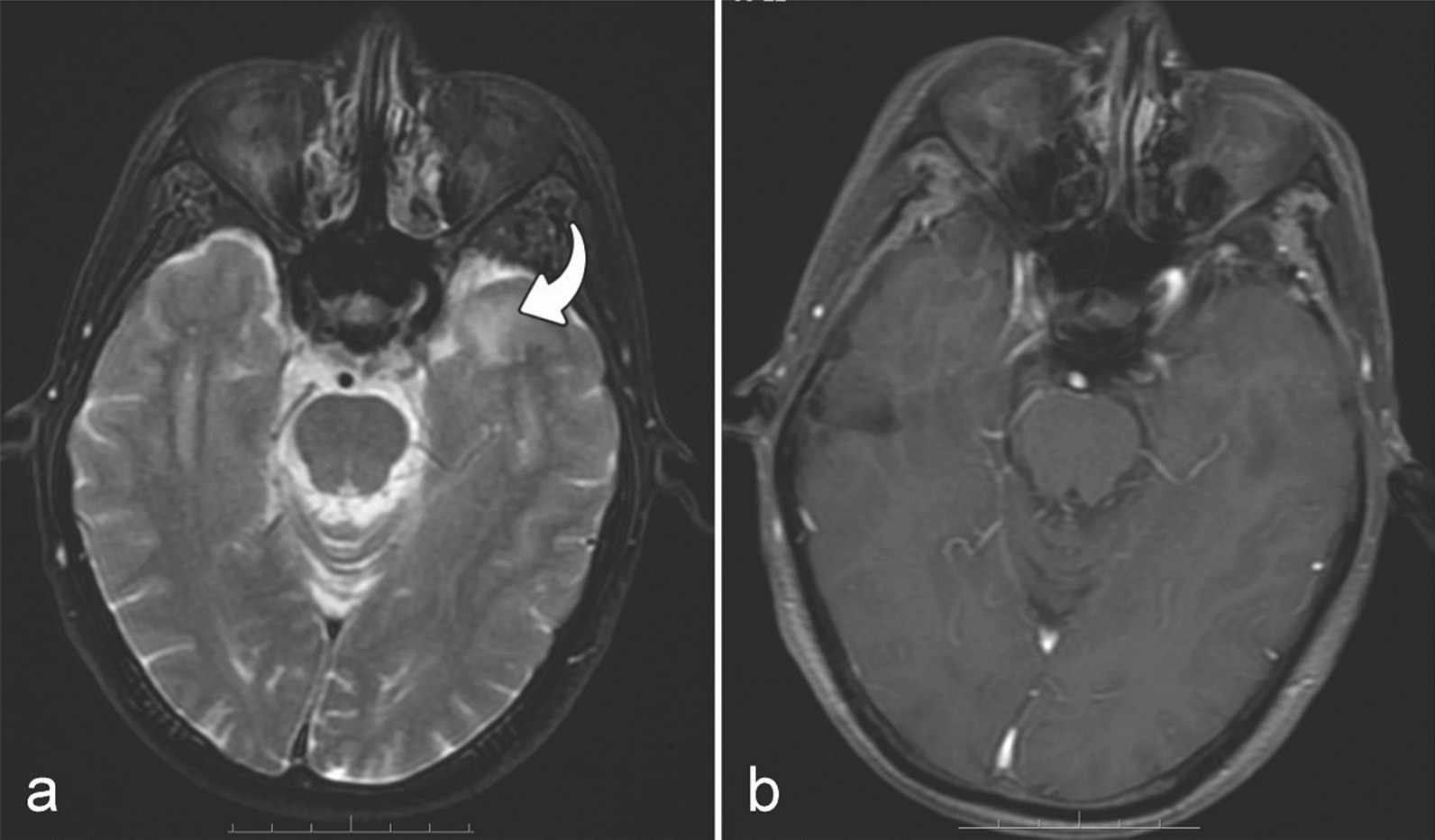
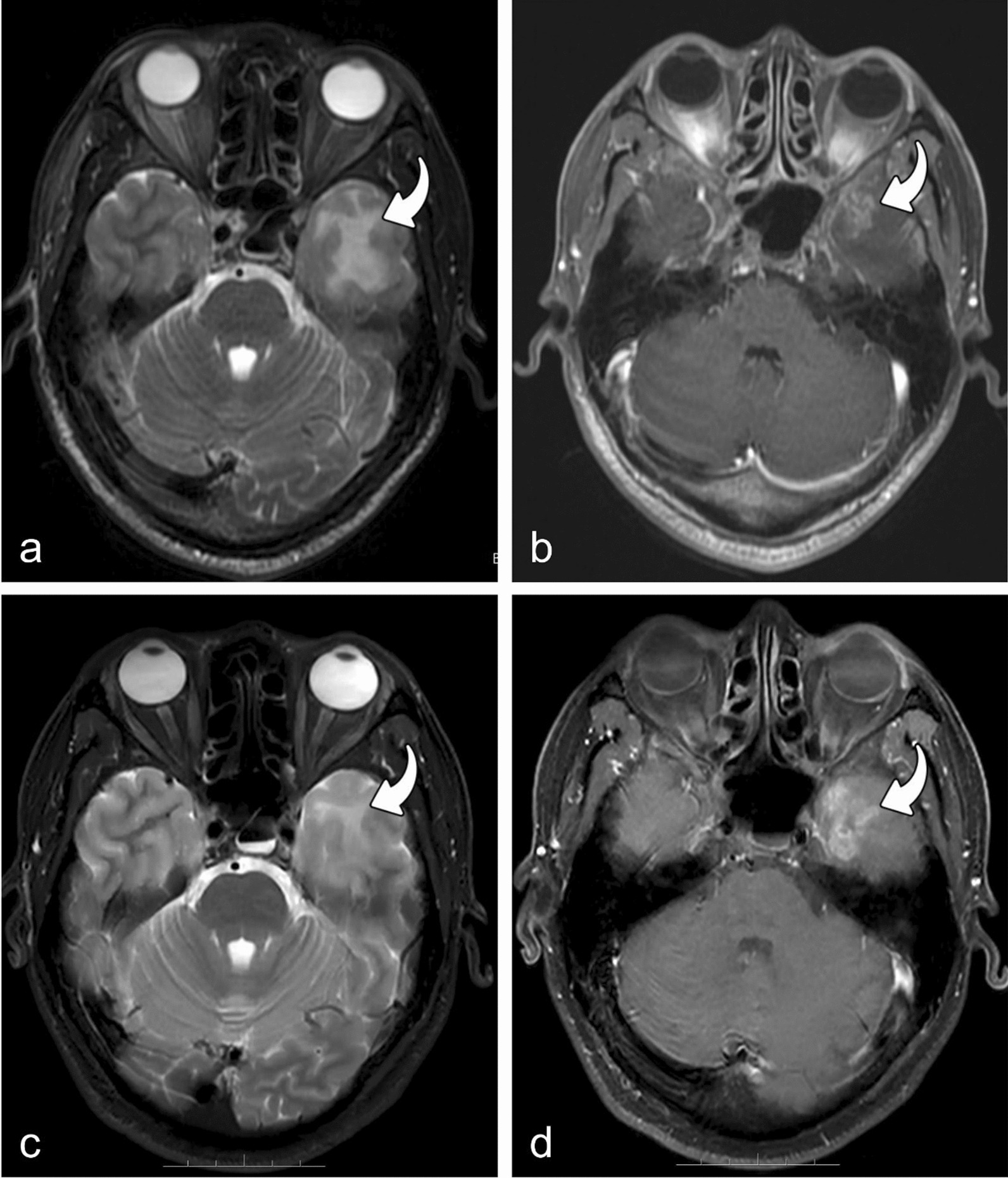
Methods: Data of patients with RTLI were retrospectively collected from two hospitals between January 2011 and December 2021. The injured lobes were categorized into three patterns based on initial MRI patterns: isolated white matter lesions (WMLs), isolated contrast-enhanced lesions (CELs), and combined WMLs and CELs. The latency period, MRI appearances, and temporal changes in WMLs and CELs were evaluated.
Results: A total of 913 RTLI patients with 1092 injured lobes were included in this study. The numbers of isolated WMLs, isolated CELs, and combined WMLs and CELs identified at the first MRI detection were 7 (0.6%), 172 (15.8%), and 913 (83.6%), respectively. The evolution of bilateral RTLI was different in the same patient, and that of unilateral RTLI combined with WMLs and CELs also may occur asynchronously. The time intervals from the initial MRI detection of isolated WMLs, isolated CELs, combined WMLs and CELs to the last negative MRI scan were 8.6, 8.9 and 11.0 months, respectively. A significant difference was observed in the time intervals between the three patterns (H = 14.287, P = 0.001). And the time interval was identified as an independent factor influencing the initial MRI pattern of RTLI after Poisson regression (P = 0.002).
Conclusion: Both WMLs and CELs could be the initial and only MRI abnormalities in patients with RTLI. This study is of great significance in accurately diagnosing RTLI early and providing timely treatment options. Additionally, it provides clinical evidence for guidelines on NPC, emphasizing the importance of regular follow-up of NPC patients.
Keywords: Intensity-modulated radiotherapy; Magnetic resonance imaging; Nasopharyngeal carcinoma; Temporal lobe injury.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures

Similar articles
-
Causes of missed MRI diagnosis of radiotherapy-induced temporal lobe injury in nasopharyngeal carcinoma.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024 May 28;49(5):698-704. doi: 10.11817/j.issn.1672-7347.2024.230574. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 39174883 Free PMC article. Chinese, English.
-
Machine-learning based MRI radiomics models for early detection of radiation-induced brain injury in nasopharyngeal carcinoma.BMC Cancer. 2020 Jun 1;20(1):502. doi: 10.1186/s12885-020-06957-4. BMC Cancer. 2020. PMID: 32487085 Free PMC article.
-
MRI-based radiomics nomogram for predicting temporal lobe injury after radiotherapy in nasopharyngeal carcinoma.Eur Radiol. 2022 Feb;32(2):1106-1114. doi: 10.1007/s00330-021-08254-5. Epub 2021 Aug 31. Eur Radiol. 2022. PMID: 34467454
-
Radiation induced temporal lobe necrosis in nasopharyngeal cancer patients after radical external beam radiotherapy.Radiat Oncol. 2020 May 15;15(1):112. doi: 10.1186/s13014-020-01560-0. Radiat Oncol. 2020. PMID: 32414378 Free PMC article. Review.
-
Radiation induced temporal lobe necrosis in patients with nasopharyngeal carcinoma: a review of new avenues in its management.Radiat Oncol. 2011 Sep 30;6:128. doi: 10.1186/1748-717X-6-128. Radiat Oncol. 2011. PMID: 21961805 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
