

Brainstem processing of cough sensory inputs in chronic cough hypersensitivity
- PMID: 38244293
- PMCID: PMC10831188
- DOI: 10.1016/j.ebiom.2024.104976
Brainstem processing of cough sensory inputs in chronic cough hypersensitivity
Abstract
Background: Chronic cough is a prevalent and difficult to treat condition often accompanied by cough hypersensitivity, characterised by cough triggered from exposure to low level sensory stimuli. The mechanisms underlying cough hypersensitivity may involve alterations in airway sensory nerve responsivity to tussive stimuli which would be accompanied by alterations in stimulus-induced brainstem activation, measurable with functional magnetic resonance imaging (fMRI).
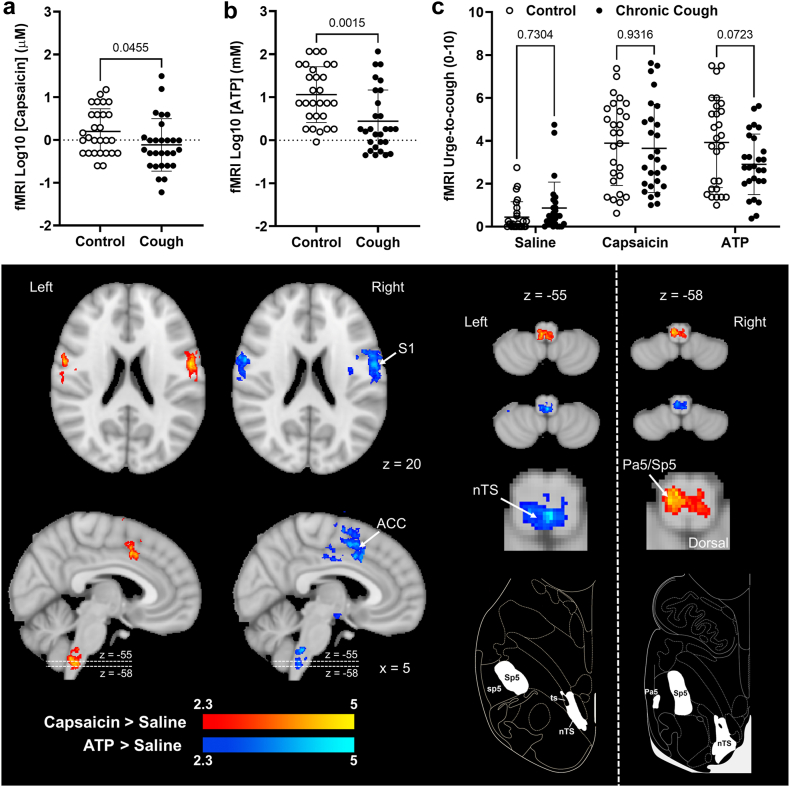
Methods: We investigated brainstem responses during inhalation of capsaicin and adenosine triphosphate (ATP) in 29 participants with chronic cough and 29 age- and sex-matched controls. Psychophysical testing was performed to evaluate individual sensitivities to inhaled stimuli and fMRI was used to compare neural activation in participants with cough and control participants while inhaling stimulus concentrations that evoked equivalent levels of urge-to-cough sensation.
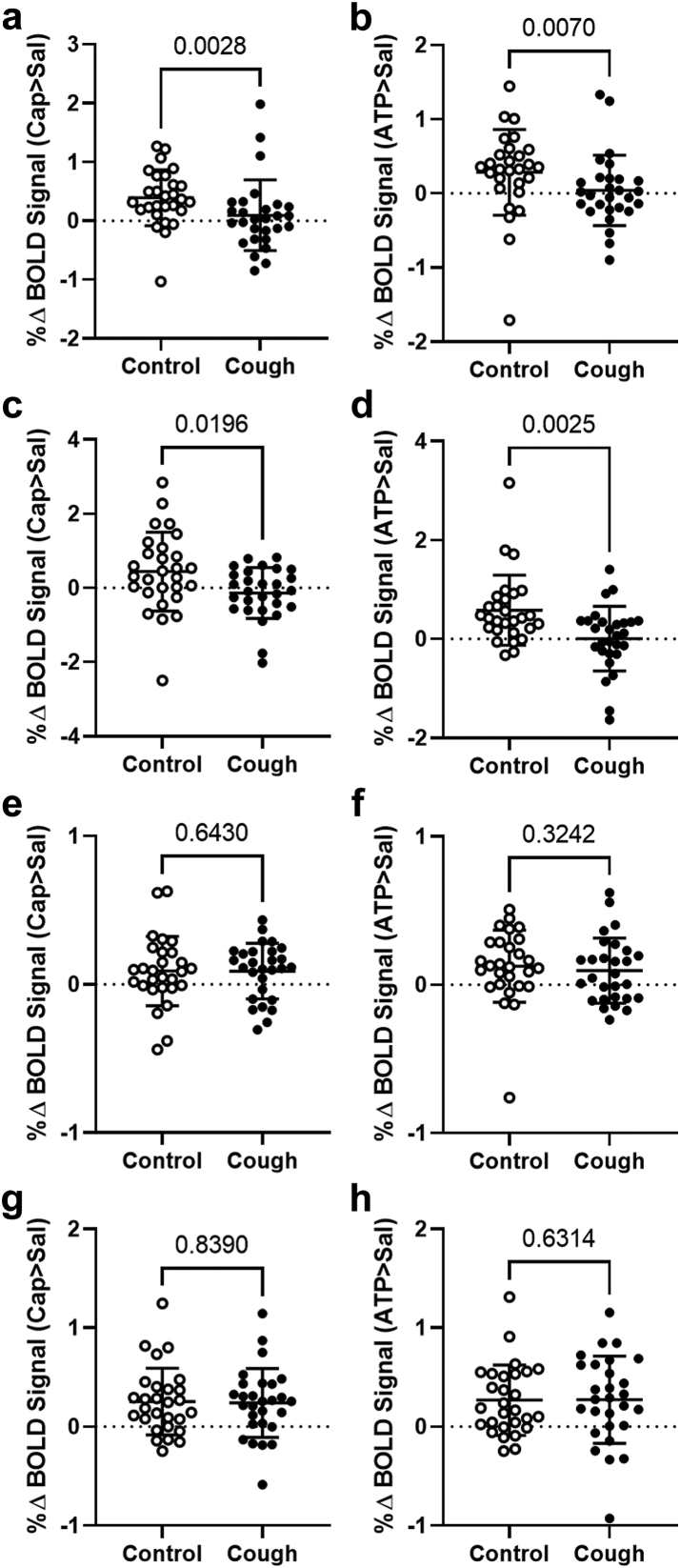
Findings: Participants with chronic cough were significantly more sensitive to inhaled capsaicin and ATP and showed a change in relationship between urge-to-cough perception and cough induction. When urge-to-cough levels were matched, participants with chronic cough displayed significantly less neural activation in medullary regions known to integrate airway sensory inputs. By contrast, neural activations did not differ significantly between the two groups in cortical brain regions known to encode cough sensations whereas activation in a midbrain region of participants with chronic cough was significantly increased compared to controls.
Interpretation: Cough hypersensitivity in some patients may occur in brain circuits above the level of the medulla, perhaps involving midbrain regions that amplify ascending sensory signals or change the efficacy of central inhibitory control systems that ordinarily serve to filter sensory inputs.
Funding: Supported in part by a research grant from Investigator-Initiated Studies Program of Merck Sharp & Dohme Pty Ltd. The opinions expressed in this paper are those of the authors and do not necessarily represent those of Merck Sharp & Dohme (Australia) Pty Ltd.
Keywords: ATP; Brain imaging; Brainstem; Cough; Purinergic; Sensitisation; Vagal sensory.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests SBM reports receiving grants from the National Health and Medical Research Council (NHMRC) of Australia and the Australian Research Council (ARC), Merck, Bellus Health and Reckitt Benkiser, and remuneration for consultancy from Merck, Trevi Therapeutics, Reckitt Benkiser and Nerre Therapeutics, has served on advisory committees for Reckitt Benkiser and has received payment from Reckitt Benkiser for assistance with manuscript writing. KFC reports research grants from Merck and GSK, remuneration for lectures from Novartis and AstraZeneca; has served on advisory boards for Roche, Merck, Reckitt Benckiser, and Shionogi & Co., Ltd., and a Data Safety Monitoring Board for Nocion. LMG reports research grants from Bayer AG, Bellus Health, Chiesi, Merck, and Shionogi, remuneration for lectures from Bayer AG, Bellus Health, Chiesi, GlaxoSmithKline, Merck, and Shionogi, remuneration for consultancy from Bayer AG, Bellus Health, Chiesi, Merck, NeRRe Therapeutics, Nocion Therapeutics, and Shionogi, and has served on advisory committees for Applied Clinical Intelligence, Bayer AG, Bellus Health, Chiesi, Merck, NeRRe Therapeutics, Nocion Therapeutics, and Shionogi and on a Data and Safety Monitoring Board for Bayer AG. All other authors declare no relevant conflict of interest.
Figures




References
-
- Song W.J., Chang Y.S., Faruqi S., et al. The global epidemiology of chronic cough in adults: a systematic review and meta-analysis. Eur Respir J. 2015;45(5):1479–1481. - PubMed
-
- Morice A.H., Faruqi S., Wright C.E., Thompson R., Bland J.M. Cough hypersensitivity syndrome: a distinct clinical entity. Lung. 2011;189(1):73–79. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
