

Genomic Landscape of Lynch Syndrome Colorectal Neoplasia Identifies Shared Mutated Neoantigens for Immunoprevention
- PMID: 38244726
- PMCID: PMC11034773
- DOI: 10.1053/j.gastro.2024.01.016
Genomic Landscape of Lynch Syndrome Colorectal Neoplasia Identifies Shared Mutated Neoantigens for Immunoprevention
Abstract
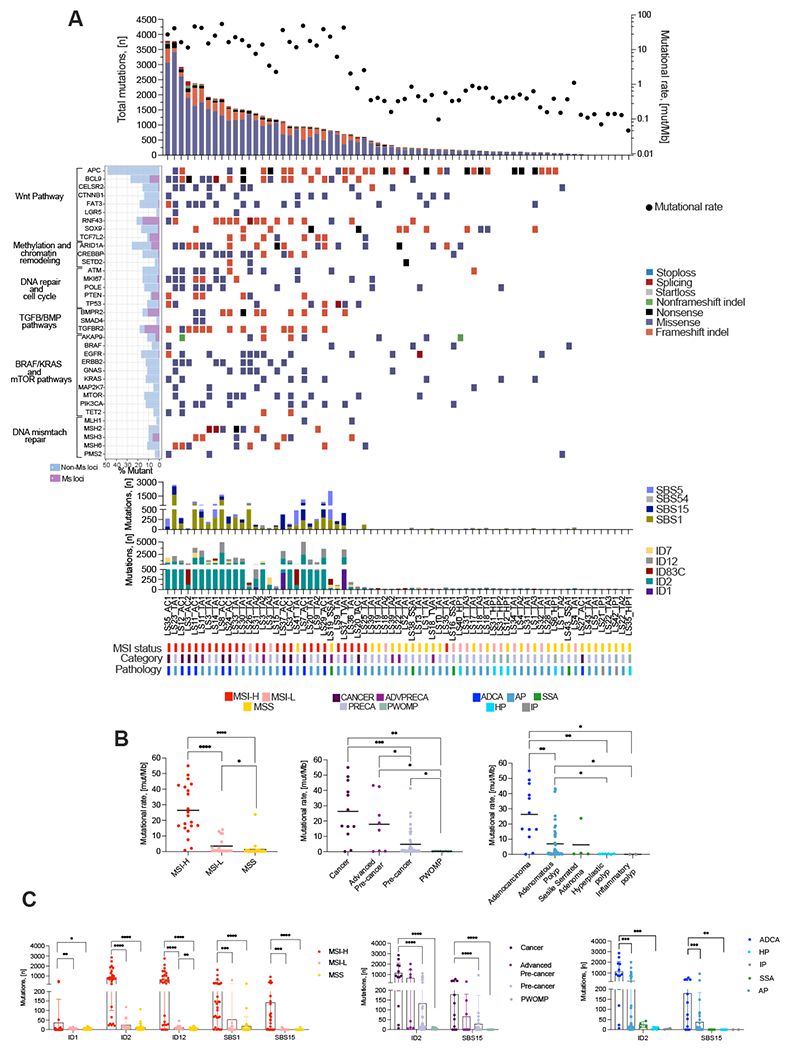
Background & aims: Lynch syndrome (LS) carriers develop mismatch repair-deficient neoplasia with high neoantigen (neoAg) rates. No detailed information on targetable neoAgs from LS precancers exists, which is crucial for vaccine development and immune-interception strategies. We report a focused somatic mutation and frameshift-neoAg landscape of microsatellite loci from colorectal polyps without malignant potential (PWOMP), precancers, and early-stage cancers in LS carriers.
Methods: We generated paired whole-exome and transcriptomic sequencing data from 8 colorectal PWOMP, 41 precancers, 8 advanced precancers, and 12 early-stage cancers of 43 LS carriers. A computational pipeline was developed to predict, rank, and prioritize the top 100 detected mutated neoAgs that were validated in vitro using ELISpot and tetramer assays.
Results: Mutation calling revealed >10 mut/Mb in 83% of cancers, 63% of advanced precancers, and 20% of precancers. Cancers displayed an average of 616 MHC-I neoAgs/sample, 294 in advanced precancers, and 107 in precancers. No neoAgs were detected in PWOMP. A total of 65% of our top 100 predicted neoAgs were immunogenic in vitro, and were present in 92% of cancers, 50% of advanced precancers, and 29% of precancers. We observed increased levels of naïve CD8+ and memory CD4+ T cells in mismatch repair-deficient cancers and precancers via transcriptomics analysis.
Conclusions: Shared frameshift-neoAgs are generated within unstable microsatellite loci at initial stages of LS carcinogenesis and can induce T-cell responses, generating opportunities for vaccine development, targeting LS precancers and early-stage cancers.
Keywords: Colorectal Cancer; Immunoprevention; Lynch Syndrome; MMR Deficiency; Neoantigen; Systems Biology.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Vilar had a consulting or advisory role with Janssen Research and Development, Recursion Pharma, Guardant Health, Rising Tide Foundation, and Nouscom AG. He has received research support from Janssen Research and Development. No disclosures were reported by the other authors.
Figures





References
-
- Lynch HT, Snyder CL, Shaw TG, et al. Milestones of Lynch syndrome: 1895-2015. Nat Rev Cancer 2015;15:181–94. - PubMed
-
- Bonadona V, Bonaiti B, Olschwang S, et al. Cancer risks associated with germline mutations in MLH1, MSH2, and MSH6 genes in Lynch syndrome. JAMA 2011;305:2304–10. - PubMed
-
- Yarchoan M, Johnson BA 3rd, Lutz ER, et al. Targeting neoantigens to augment antitumour immunity. Nat Rev Cancer 2017;17:569. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
