

Evaluation of the Xpert MTB Host Response assay for the triage of patients with presumed pulmonary tuberculosis: a prospective diagnostic accuracy study in Viet Nam, India, the Philippines, Uganda, and South Africa
- PMID: 38245113
- PMCID: PMC11046618
- DOI: 10.1016/S2214-109X(23)00541-7
Evaluation of the Xpert MTB Host Response assay for the triage of patients with presumed pulmonary tuberculosis: a prospective diagnostic accuracy study in Viet Nam, India, the Philippines, Uganda, and South Africa
Abstract
Background: Non-sputum-based triage tests for tuberculosis are a priority for ending tuberculosis. We aimed to evaluate the diagnostic accuracy of the late-prototype Xpert MTB Host Response (Xpert HR) blood-based assay.
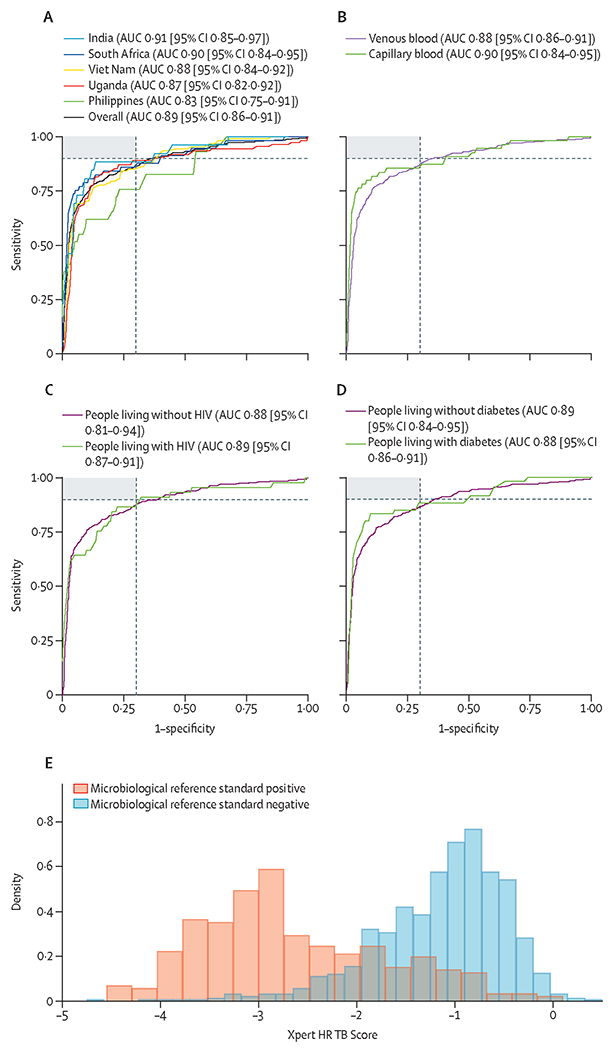
Methods: We conducted a prospective diagnostic accuracy study among outpatients with presumed tuberculosis in outpatient clinics in Viet Nam, India, the Philippines, Uganda, and South Africa. Eligible participants were aged 18 years or older and reported cough lasting at least 2 weeks. We excluded those receiving tuberculosis treatment in the preceding 12 months and those who were unwilling to consent. Xpert HR was performed on capillary or venous blood. Reference standard testing included sputum Xpert MTB/RIF Ultra and mycobacterial culture. We performed receiver operating characteristic (ROC) analysis to identify the optimal cutoff value for the Xpert HR to achieve the target sensitivity of 90% or more while maximising specificity, then calculated diagnostic accuracy using this cutoff value. This study was prospectively registered with ClinicalTrials.gov, NCT04923958.
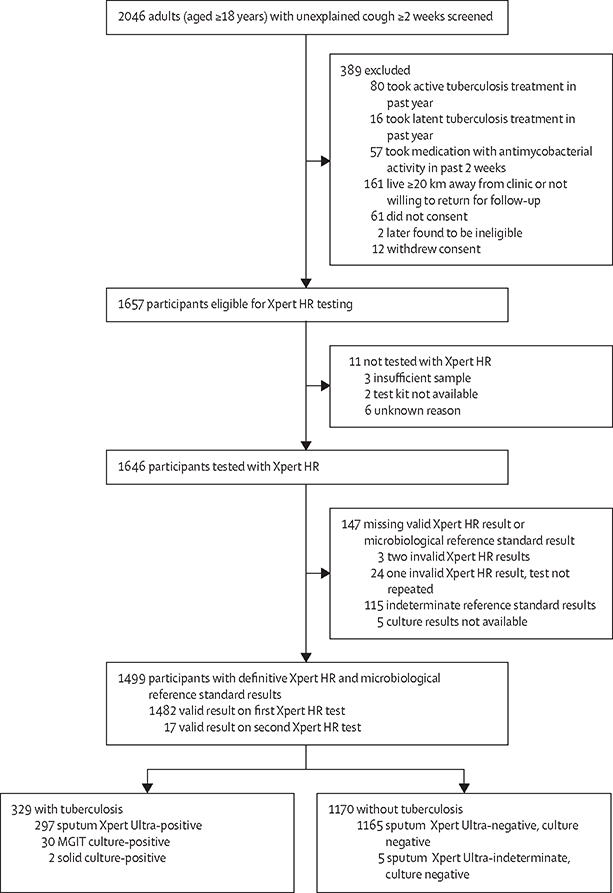
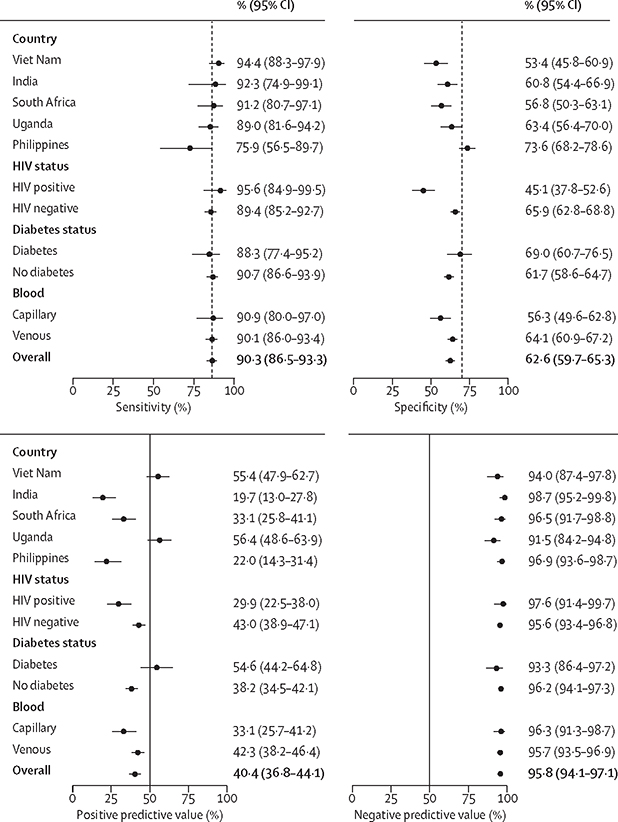
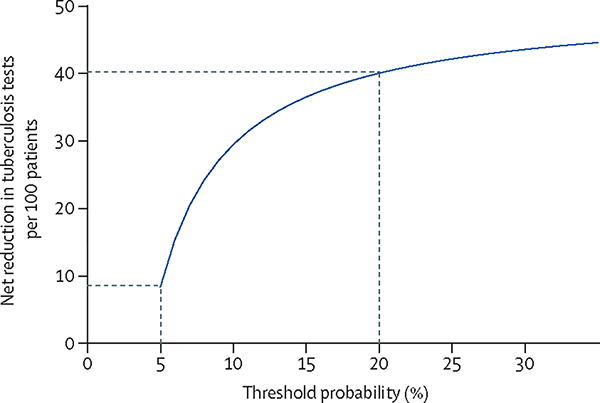
Findings: Between July 13, 2021, and Aug 15, 2022, 2046 adults with at least 2 weeks of cough were identified, of whom 1499 adults (686 [45·8%] females and 813 [54·2%] males) had valid Xpert HR and reference standard results. 329 (21·9%) had microbiologically confirmed tuberculosis. Xpert HR had an area under the ROC curve of 0·89 (95% CI 0·86-0·91). The optimal cutoff value was less than or equal to -1·25, giving a sensitivity of 90·3% (95% CI 86·5-93·3; 297 of 329) and a specificity of 62·6% (95% CI 59·7-65·3; 732 of 1170). Sensitivity was similar across countries, by sex, and by subgroups, although specificity was lower in people living with HIV (45·1%, 95% CI 37·8-52·6) than in those not living with HIV (65·9%, 62·8-68·8; difference of 20·8%, 95% CI 13·0-28·6; p<0·0001). Xpert HR had high negative predictive value (95·8%, 95% CI 94·1-97·1), but positive predictive value was only 40·1% (95% CI 36·8-44·1). Using the Xpert HR as a triage test would have reduced confirmatory sputum testing by 57·3% (95% CI 54·2-60·4).
Interpretation: Xpert HR did not meet WHO minimum specificity targets for a non-sputum-based triage test for pulmonary tuberculosis. Despite promise as a rule-out test that could reduce confirmatory sputum testing, further cost-effectiveness modelling and data on acceptability and usability are needed to inform policy recommendations.
Funding: National Institute of Allergy and Infectious Diseases of the US National Institutes of Health.
Translations: For the Vietnamese and Tagalog translations of the abstract see Supplementary Materials section.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests CMD, PPJP, AC, and GT declare support from the underlying R2D2 TB Network to their institutions from the National Institute of Allergy and Infectious Diseases of the US National Institutes of Health (NIH). CMD also declares research grants from the German Ministry of Education and Research, German Alliance for Global Health Research, US Agency for International Development, FIND, German Center for Infection Research, and WHO. GT declares donations of reagents and equipment by Cepheid for other projects. AC declares research funding to his institution from NIH, Bill and Melinda Gates Foundation, and Global Health Labs. All other authors declare no competing interests.
Figures
Comment in
-
Triage test to diagnose presumptive pulmonary tuberculosis.Lancet Glob Health. 2024 Feb;12(2):e175-e176. doi: 10.1016/S2214-109X(23)00604-6. Lancet Glob Health. 2024. PMID: 38245104 No abstract available.
References
-
- WHO. Global tuberculosis report 2023. Geneva: World Health Organization, 2023.
-
- WHO. The end TB strategy. Global strategy and targets for tuberculosis prevention, care and control after 2015. Geneva: World Health Organization, 2014.
-
- WHO. Report: Consensus meeting on high-priority target product profiles, 28–29th April 2014. Geneva: World Health Organization, 2014.
