

Adjuvant Therapy for Patients with a Tumor-Positive Resection Margin After Neoadjuvant Chemoradiotherapy and Esophagectomy
- PMID: 38245648
- PMCID: PMC11076321
- DOI: 10.1245/s10434-024-14912-x
Adjuvant Therapy for Patients with a Tumor-Positive Resection Margin After Neoadjuvant Chemoradiotherapy and Esophagectomy
Abstract
Background: Approximately 4-9% of patients have a tumor-positive resection margin after neoadjuvant chemoradiotherapy (nCRT) and esophagectomy. Although it is associated with decreased survival, Western guidelines do not recommend adjuvant treatment.
Objective: The aim of this study was to assess the proportion of patients who received adjuvant therapy, and to evaluate overall survival (OS) after esophagectomy in patients with a tumor-positive resection margin.
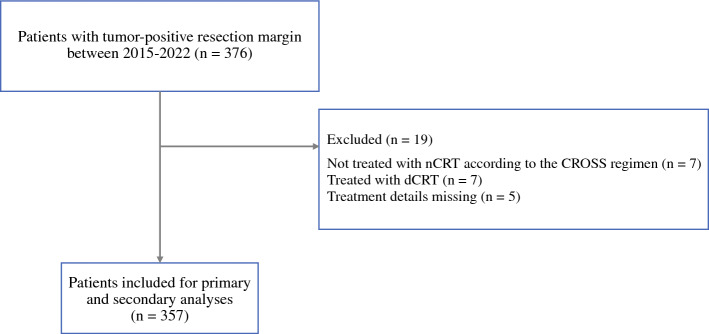
Methods: Patients diagnosed with resectable (cT2-4a/cTxN0-3/NxM0) esophageal cancer between 2015 and 2022, and treated with nCRT followed by irradical esophagectomy, were selected from the Netherlands Cancer Registry. The primary outcome was the proportion of patients with a tumor-positive resection margin who started adjuvant treatment ≤16 weeks after esophagectomy, including chemotherapy/radiotherapy, immunotherapy, or targeted therapy. OS was calculated from the date of surgery until the date of death or last day of follow-up.
Results: Overall, 376 patients were included in our study, of whom 357 were treated with nCRT. Of these 357 patients, 98.3% had a microscopically irradical resection and 1.7% had a macroscopically irradical resection. Approximately 72.3% of tumors showed a partial response (Mandard 2-3) and 11.8% showed little/no pathological response (Mandard 4-5) to nCRT. One of 357 patients underwent adjuvant chemoradiotherapy and 39 patients (61%) underwent adjuvant immunotherapy (nivolumab). The median and 5-year OS rate of all patients was 16.4 months (95% confidence interval 13.1-19.8) and 21%, respectively.
Conclusion: Real-world population-level data showed that no patients with a tumor-positive resection margin underwent adjuvant therapy following nCRT and esophagectomy prior to 2021. Interestingly, 61% of patients were treated with adjuvant nivolumab in 2021-2022. OS after irradical esophagectomy is poor and long-term data will explore the added value of nivolumab.
Keywords: Adjuvant therapy; Esophageal cancer; Neoadjuvant chemoradiotherapy; Tumor-positive resection margin.
© 2024. The Author(s).
Conflict of interest statement
Bianca Mostert has received research funding from Sanofi, Pfizer and BMS, and undertaken consulting/advisory roles for Lilly, Servier, BMS, Amgen and AstraZeneca. Bas P.L. Wijnhoven has received research funding from BMS, and undertaken consulting/advisory roles for BMS. Charlène J. van der Zijden, Pieter C. van der Sluis, Joost J.M.E. Nuyttens, Manon C.W. Spaander, Roelf Valkema, Jelle P. Ruurda, and Sjoerd M. Lagarde have declared no conflicts of interest.
Figures
References
-
- Shapiro J, van Lanschot JJB, Hulshof M, van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–1098. doi: 10.1016/S1470-2045(15)00040-6. - DOI - PubMed
-
- Defize IL, Goense L, Borggreve AS, Mook S, Meijer GJ, Ruurda JP, et al. Risk factors for tumor positive resection margins after neoadjuvant chemoradiotherapy for esophageal cancer: results from the dutch upper GI cancer audit: a nationwide population-based study. Ann Surg. 2023;277(2):e313–e319. doi: 10.1097/SLA.0000000000005112. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
