

Myoelectric interface for neurorehabilitation conditioning to reduce abnormal leg co-activation after stroke: a pilot study
- PMID: 38245730
- PMCID: PMC10800046
- DOI: 10.1186/s12984-024-01305-0
Myoelectric interface for neurorehabilitation conditioning to reduce abnormal leg co-activation after stroke: a pilot study
Abstract
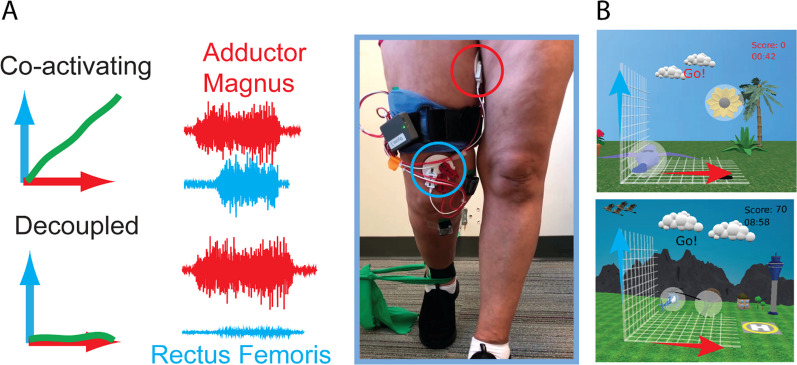
Background: The ability to walk is an important factor in quality of life after stroke. Co-activation of hip adductors and knee extensors has been shown to correlate with gait impairment. We have shown previously that training with a myoelectric interface for neurorehabilitation (MINT) can reduce abnormal muscle co-activation in the arms of stroke survivors.
Methods: Here, we extend MINT conditioning to stroke survivors with leg impairment. The aim of this pilot study was to assess the safety and feasibility of using MINT to reduce abnormal co-activation between hip adductors and knee extensors and assess any effects on gait. Nine stroke survivors with moderate to severe gait impairment received 6 h of MINT conditioning over six sessions, either in the laboratory or at home.
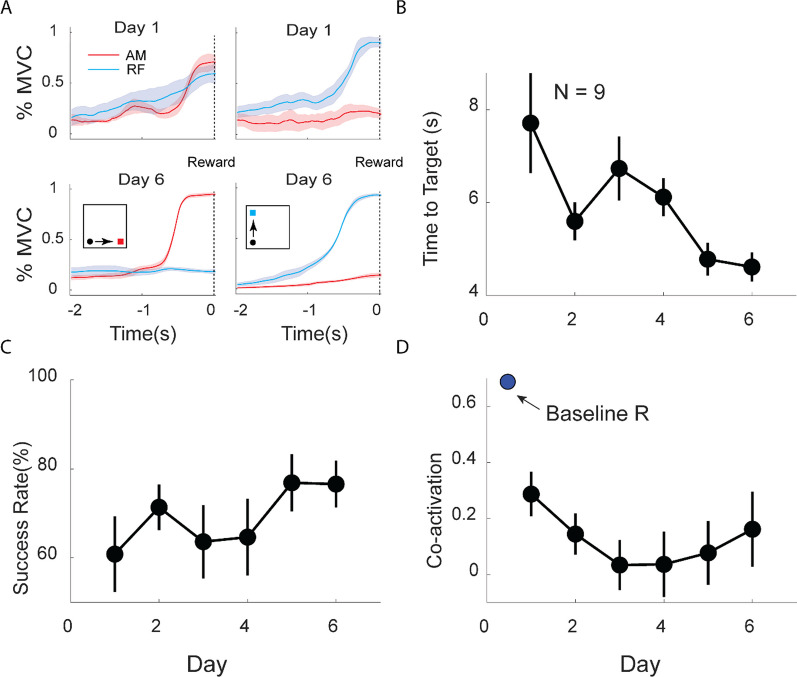
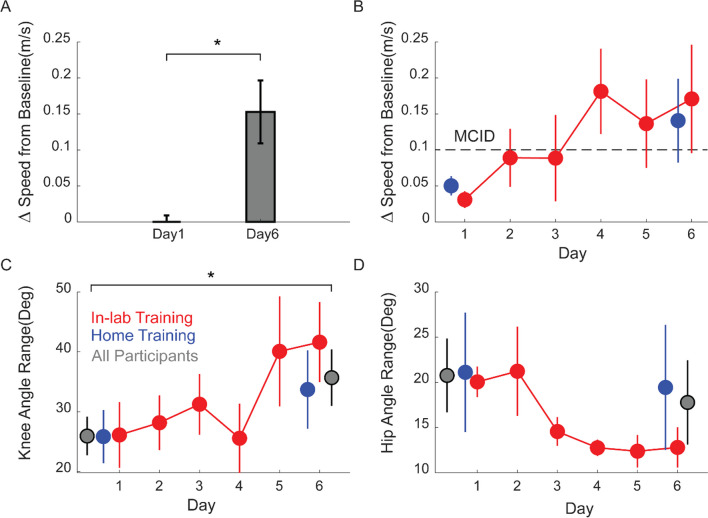
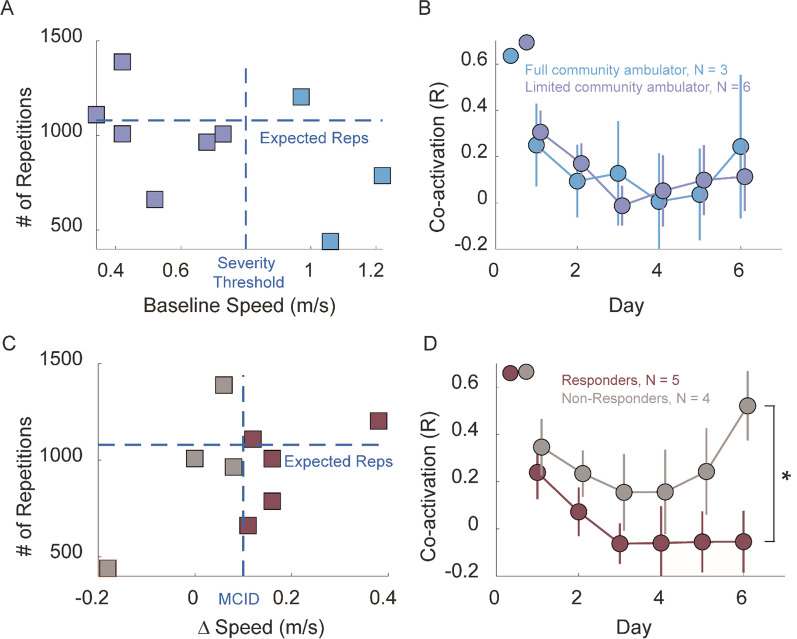
Results: MINT participants completed a mean of 159 repetitions per session without any adverse events. Further, participants learned to isolate their muscles effectively, resulting in a mean reduction of co-activation of 70% compared to baseline. Moreover, gait speed increased by a mean of 0.15 m/s, more than the minimum clinically important difference. Knee flexion angle increased substantially, and hip circumduction decreased.
Conclusion: MINT conditioning is safe, feasible at home, and enables reduction of co-activation in the leg. Further investigation of MINT's potential to improve leg movement and function after stroke is warranted. Abnormal co-activation of hip adductors and knee extensors may contribute to impaired gait after stroke. Trial registration This study was registered at ClinicalTrials.gov (NCT03401762, Registered 15 January 2018, https://clinicaltrials.gov/study/NCT03401762?tab=history&a=4 ).
Keywords: Co-activation; EMG; Gait; Game-based rehabilitation; Knee flexion; Stroke.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they do not have any conflicts of interest concerning the research, authorship, and/or publication of this article.
Figures
Update of
-
Myoelectric interface for neurorehabilitation conditioning to reduce abnormal leg co-activation after stroke: a pilot study.Res Sq [Preprint]. 2023 Oct 9:rs.3.rs-3398815. doi: 10.21203/rs.3.rs-3398815/v1. Res Sq. 2023. Update in: J Neuroeng Rehabil. 2024 Jan 20;21(1):11. doi: 10.1186/s12984-024-01305-0. PMID: 37886579 Free PMC article. Updated. Preprint.
Similar articles
-
Wearable Myoelectric Interface for Neurorehabilitation (MINT) to Recover Arm Function: a Randomized Controlled Trial.medRxiv [Preprint]. 2025 Jun 25:2025.06.24.25330240. doi: 10.1101/2025.06.24.25330240. medRxiv. 2025. PMID: 40666333 Free PMC article. Preprint.
-
Myoelectric interface for neurorehabilitation conditioning to reduce abnormal leg co-activation after stroke: a pilot study.Res Sq [Preprint]. 2023 Oct 9:rs.3.rs-3398815. doi: 10.21203/rs.3.rs-3398815/v1. Res Sq. 2023. Update in: J Neuroeng Rehabil. 2024 Jan 20;21(1):11. doi: 10.1186/s12984-024-01305-0. PMID: 37886579 Free PMC article. Updated. Preprint.
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Virtual reality for stroke rehabilitation.Cochrane Database Syst Rev. 2025 Jun 20;6(6):CD008349. doi: 10.1002/14651858.CD008349.pub5. Cochrane Database Syst Rev. 2025. PMID: 40537150 Free PMC article.
-
Music interventions for acquired brain injury.Cochrane Database Syst Rev. 2017 Jan 20;1(1):CD006787. doi: 10.1002/14651858.CD006787.pub3. Cochrane Database Syst Rev. 2017. PMID: 28103638 Free PMC article.
Cited by
-
Wearable Myoelectric Interface for Neurorehabilitation (MINT) to Recover Arm Function: a Randomized Controlled Trial.medRxiv [Preprint]. 2025 Jun 25:2025.06.24.25330240. doi: 10.1101/2025.06.24.25330240. medRxiv. 2025. PMID: 40666333 Free PMC article. Preprint.
-
Active Dissociation of Intracortical Spiking and High Gamma Activity.bioRxiv [Preprint]. 2025 Jul 11:2025.07.10.663559. doi: 10.1101/2025.07.10.663559. bioRxiv. 2025. PMID: 40672280 Free PMC article. Preprint.
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
