

Prone positioning effect on tracheal intubation rate, mortality and oxygenation parameters in awake non-intubated severe COVID-19-induced respiratory failure: a review of reviews
- PMID: 38245784
- PMCID: PMC10799467
- DOI: 10.1186/s40001-024-01661-6
Prone positioning effect on tracheal intubation rate, mortality and oxygenation parameters in awake non-intubated severe COVID-19-induced respiratory failure: a review of reviews
Abstract
Background: Prone positioning (PP) is a low-cost method with minimal risk to the patient that improves the oxygenation of patients with acute hypoxic respiratory failure (AHRF) due to COVID-19 pneumonia, thereby reducing their need for tracheal intubation (TI) and transferring to the intensive care unit (ICU). We aimed to overview the results of all previous systematic reviews and meta-analyses to examine the net effect of PP on oxygenation, the rate of TI and mortality in COVID-19 patients.
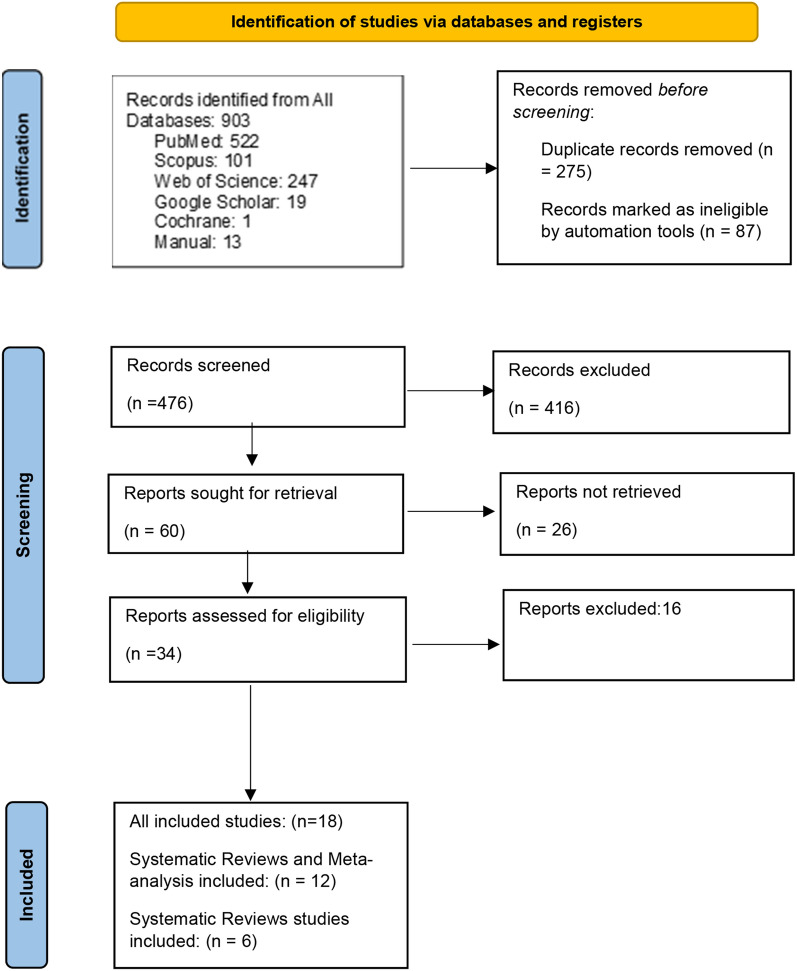
Methods: We searched PubMed, Scopus, Web of Science, Google Scholar, and Cochrane Library databases from December 2019 through 2022 without publication language restriction for systematic reviews and meta-analysis studies on PP vs. supine position (SP) in conscious patients with hypoxic respiratory failure COVID-19. After study selection, data were extracted from published meta-analyses and pooled by comprehensive meta-analysis (CMA) software version 2.2.064 to achieve effect sizes. They were analyzed for TI and mortality rates dichotomous variables, and the results were shown as pooled odds ratios (OR) with a 95% confidence interval (CI). Continuous variables such as oxygenation indices (PaO2/FiO2 and SpO2) were also analyzed, and the data were shown as mean differences (MD) with lower and upper CI. The level of statistical significance was set at p ≤ 0.05.
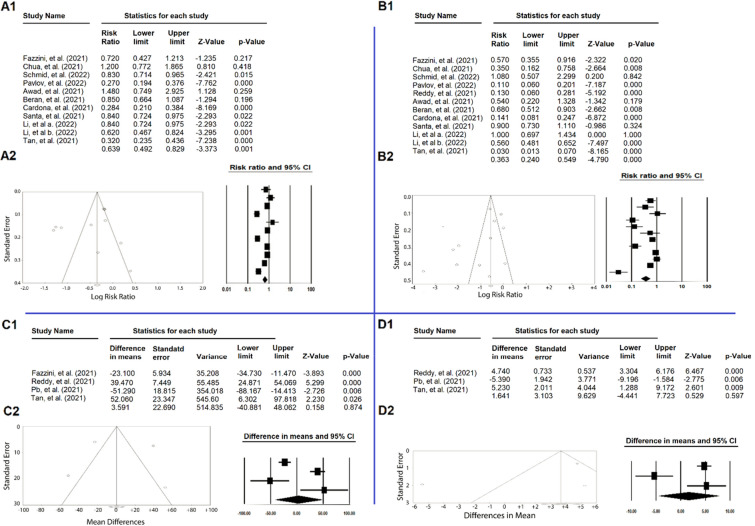
Results: Twelve systematic reviews and meta-analyses with 19,651 patients and six systematic reviews with 2,911 patients were included in this Review of Reviews (total: 22,562). PP treatment significantly reduced the rate of TI (OR = 0.639, %95 CI (0.492, 0.829); P-value = 0.001) and decreased mortality (OR = 0.363, %95 CI (0.240, 0.549), P-value < 0.001). There was no difference in PaO2/FiO2 (MD = 3.591[- 40.881, 48.062]; P-value = 0.874) and SpO2 percent (MD = 1.641[- 4.441, 7.723]; P-value = 0.597).
Conclusion: Prone positioning can be recommended in conscious ICU patients with COVID-19 pneumonia to reduce mortality and intubation.
Systematic review registration: PROSPERO registration number: CRD42022326951. Registered 25 April 2022.
Keywords: Acute hypoxic respiratory failure; Awake; COVID-19; Prone position; Supine position.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Prone position for acute respiratory failure in adults.Cochrane Database Syst Rev. 2015 Nov 13;2015(11):CD008095. doi: 10.1002/14651858.CD008095.pub2. Cochrane Database Syst Rev. 2015. PMID: 26561745 Free PMC article.
-
Positioning for acute respiratory distress in hospitalised infants and children.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD003645. doi: 10.1002/14651858.CD003645.pub4. Cochrane Database Syst Rev. 2022. PMID: 35661343 Free PMC article.
-
High-flow nasal cannulae for respiratory support in adult intensive care patients.Cochrane Database Syst Rev. 2017 May 30;5(5):CD010172. doi: 10.1002/14651858.CD010172.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2021 Mar 4;3:CD010172. doi: 10.1002/14651858.CD010172.pub3. PMID: 28555461 Free PMC article. Updated.
-
Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2017 Jul 13;7(7):CD004104. doi: 10.1002/14651858.CD004104.pub4. Cochrane Database Syst Rev. 2017. PMID: 28702957 Free PMC article.
-
Effect of mechanical ventilation in the prone position on clinical outcomes in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis.CMAJ. 2008 Apr 22;178(9):1153-61. doi: 10.1503/cmaj.071802. CMAJ. 2008. PMID: 18427090 Free PMC article.
Cited by
-
Therapeutic Impact of Tocilizumab in the Setting of Severe COVID-19; an Updated and Comprehensive Review on Current Evidence.Arch Acad Emerg Med. 2024 May 9;12(1):e47. doi: 10.22037/aaem.v12i1.2217. eCollection 2024. Arch Acad Emerg Med. 2024. PMID: 38994467 Free PMC article.
-
Nursing Practice of Airway Care Interventions and Prone Positioning in ICU Patients with COVID-19-A Dutch National Survey.J Clin Med. 2024 Mar 29;13(7):1983. doi: 10.3390/jcm13071983. J Clin Med. 2024. PMID: 38610748 Free PMC article.
-
Guideline on positioning and early mobilisation in the critically ill by an expert panel.Intensive Care Med. 2024 Aug;50(8):1211-1227. doi: 10.1007/s00134-024-07532-2. Epub 2024 Jul 29. Intensive Care Med. 2024. PMID: 39073582
-
Longer ICU stay and invasive mechanical ventilation accelerate telomere shortening in COVID-19 patients 1 year after recovery.Crit Care. 2024 Aug 7;28(1):267. doi: 10.1186/s13054-024-05051-6. Crit Care. 2024. PMID: 39113075 Free PMC article.
References
-
- Shahsavarinia K, Ghojazadeh M, Ghabousian A, Hatefnia F, Soleimanpour M, Soleimanpour H. An umbrella review of clinical efficacy and adverse cardiac events associated with hydroxychloroquine or chloroquine with or without azithromycin in patients with COVID-19. Anesth Pain Med. 2021;11(4):e115827. doi: 10.5812/aapm.115827. - DOI - PMC - PubMed
-
- Shahsavarinia K, Ghojazadeh M, Sanaie S, Vahedi L, Ahmadpour M, Mahmoodpoor A, et al. Clinical efficacy of hydroxychloroquine or chloroquine in patients with COVID-19: an umbrella review. Pharm Sci. 2021;27(4):481–488.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
