

Strategy for acute DeBakey type I aortic dissection considering midterm results: a retrospective cohort study comparing ascending aortic replacement and total arch replacement with frozen elephant trunk technique
- PMID: 38247014
- PMCID: PMC10801927
- DOI: 10.1186/s13019-024-02484-6
Strategy for acute DeBakey type I aortic dissection considering midterm results: a retrospective cohort study comparing ascending aortic replacement and total arch replacement with frozen elephant trunk technique
Abstract
Background: Acute type A aortic dissection is treated with an emergency procedure that uses ascending aortic replacement (AAR). However, to avoid a residual dissected aorta with a false lumen, total arch replacement (TAR) is required. The frozen elephant trunk (FET) technique is a promising surgical approach that promotes false lumen obliteration in a single step. Therefore, this retrospective single-center study aimed to evaluate the operative outcomes of AAR and TAR with FET.
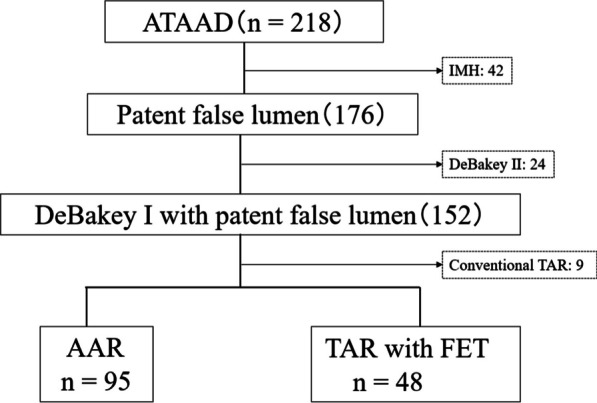
Methods: Between 2007 and 2021, 143 patients with acute DeBakey type I aortic dissection underwent a central repair using AAR (n = 95) or TAR with FET (n = 43). All perioperative variables, the duration of all-cause mortality, and aortic events defined as dilatation of the distal aorta > 5 cm, new occurrences of aortic dissection, distal aortic surgery, and distal aortic rupture were recorded. We compared these perioperative variables and mid-term results with an additional focus on distal aortic events.
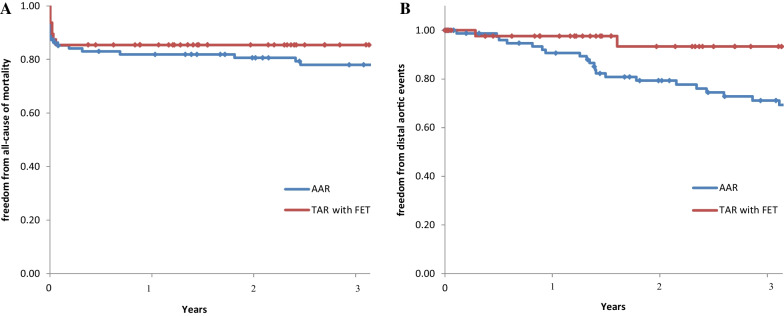
Results: Patient background data did not differ between the two groups. Perioperative results for the TAR with FET group vs the AAR group showed similar operative times (306 vs 298 min, P = 0.862), but the TAR group had longer cardiopulmonary bypass times (154 vs 179 min, P < 0.001). The freedom from all-cause death for the TAR vs AAR groups using the Kaplan-Meier method was 81.9% vs 85.4% and 78.0% vs 85.4% (P = 0.407) at 1 and 3 years, respectively. Freedom from aorta-related events was 90.6% vs 97.6% and 69.3% vs 87.0% (P = 0.034) at 1 and 3 years, respectively.
Conclusions: TAR with FET had comparable perioperative results to AAR in acute DeBakey type I aortic dissection and was considered a valuable method to avoid aorta-related events in the midterm.
Keywords: Aortic dissection; Ascending aortic replacement; Frozen elephant trunk technique; Total arch replacement.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
