Ozonated Sunflower Oil (OSO) Alleviates Inflammatory Responses in Oxazolone-Induced Atopic Dermatitis (AD)-Like Mice and LPS-Treated RAW 264.7 Cells
- PMID: 38247218
- PMCID: PMC11091665
- DOI: 10.4014/jmb.2310.10037
Ozonated Sunflower Oil (OSO) Alleviates Inflammatory Responses in Oxazolone-Induced Atopic Dermatitis (AD)-Like Mice and LPS-Treated RAW 264.7 Cells
Abstract
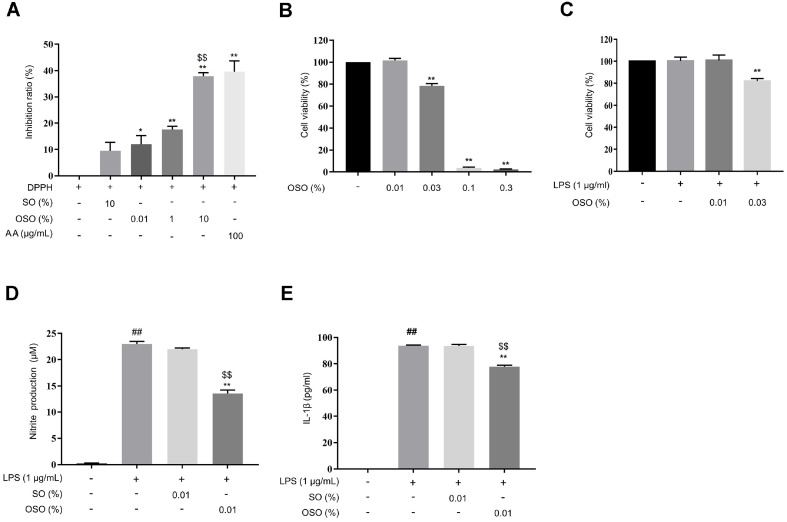
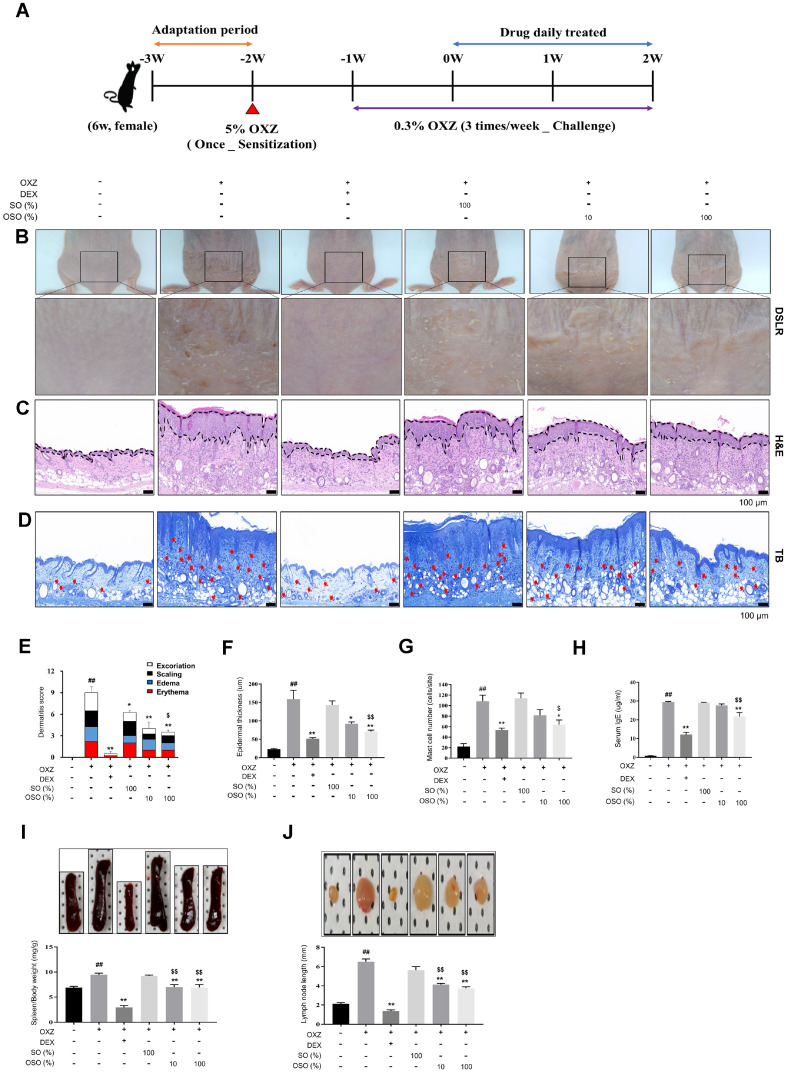
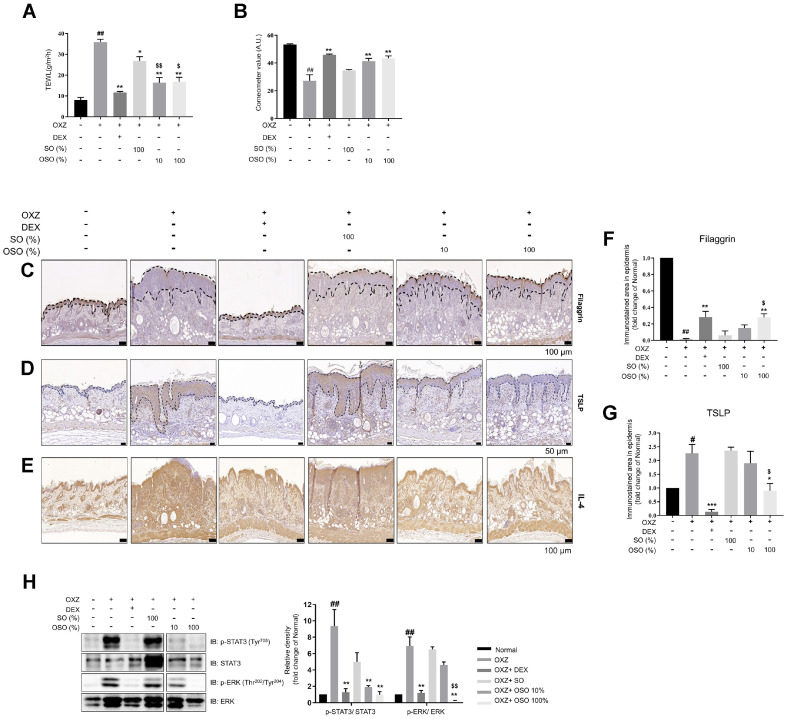
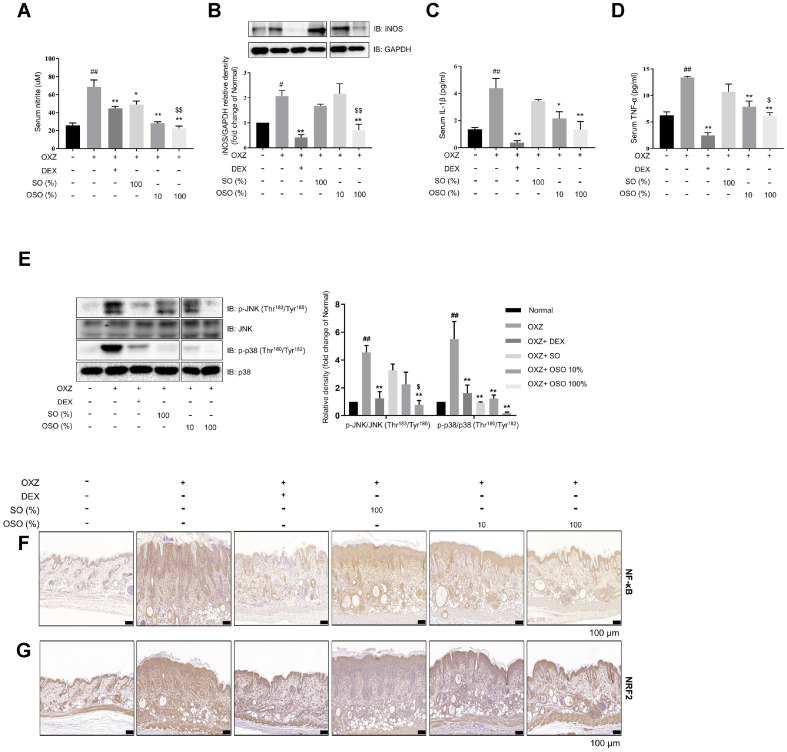
Ozone, a highly reactive oxidant molecule, is widely used as a complementary therapy for various skin diseases, including wound healing, pressure ulcers, diabetic foot, and infections. However, there is limited research on the effectiveness of ozone for atopic dermatitis (AD). Ozonated sunflower oil (OSO) is an active ingredient obtained from partially ozonated sunflower oil (SO). OSO markedly reduced the LPS-induced increase in IL-1β and nitric oxide (NO) levels in RAW 264.7 mouse macrophage cells. Oxazolone (OXZ) was applied to hairless mice to induce AD-like skin symptoms and immune response. OSO significantly alleviated the OXZ-induced increases in the number of infiltrating mast cells, epidermal thickness, AD symptoms, thymic stromal lymphopoietin (TSLP), and filaggrin, as well as the serum levels of NO, IgE, IL-1β, and TNF-α. Furthermore, OSO inhibited the IL-4/STAT3/MAPK pathway and the expression of NF-κB. Our results suggest that OSO treatment could relieve AD-mediated skin damage through its anti-inflammatory and antioxidant activities. Therefore, it can be used as a therapeutic agent against AD-related skin diseases.
Keywords: Atopic dermatitis (AD); Ozonated sunflower oil (OSO); RAW 264.7; TSLP; filaggrin; inflammation.
Conflict of interest statement
The authors have no financial conflicts of interest to declare.
Figures
Similar articles
-
Efficacy and action mechanisms of a Chinese herbal formula on experimental models of atopic dermatitis.J Ethnopharmacol. 2021 Jun 28;274:114021. doi: 10.1016/j.jep.2021.114021. Epub 2021 Mar 11. J Ethnopharmacol. 2021. PMID: 33716079
-
Ameliorative Effects of Escin on Inflammation via Glucocorticoid Receptor (GR) in Atopic Dermatitis (AD) Mouse Model.J Microbiol Biotechnol. 2025 Mar 11;35:e2410025. doi: 10.4014/jmb.2410.10025. J Microbiol Biotechnol. 2025. PMID: 40081901 Free PMC article.
-
Dendrobium officinale Kimura et Migo polysaccharide ameliorated DNFB-induced atopic dermatitis in mice associated with suppressing MAPK/NF-κB/STAT3 signaling pathways.J Ethnopharmacol. 2024 Dec 5;335:118677. doi: 10.1016/j.jep.2024.118677. Epub 2024 Aug 8. J Ethnopharmacol. 2024. PMID: 39121927
-
FGF-21 fusion proteins ameliorate atopic dermatitis by inhibiting the TLR/TSLP signaling pathway: Anti-inflammatory and skin barrier repair effects.Int Immunopharmacol. 2025 Jun 26;159:114920. doi: 10.1016/j.intimp.2025.114920. Epub 2025 May 26. Int Immunopharmacol. 2025. PMID: 40424659 Review.
-
Rodent models to evaluate the impact of cadmium exposure on atopic dermatitis.Ital J Dermatol Venerol. 2025 Jun;160(3):262-276. doi: 10.23736/S2784-8671.25.08133-2. Ital J Dermatol Venerol. 2025. PMID: 40485577 Review.
Cited by
-
Multiplicative Effects of Essential Oils and Other Active Components on Skin Tissue and Skin Cancers.Int J Mol Sci. 2024 May 15;25(10):5397. doi: 10.3390/ijms25105397. Int J Mol Sci. 2024. PMID: 38791435 Free PMC article. Review.
-
Topical ozone in atopic dermatitis: a viable treatment option?Arch Dermatol Res. 2025 Feb 1;317(1):330. doi: 10.1007/s00403-025-03855-2. Arch Dermatol Res. 2025. PMID: 39893255 No abstract available.
-
Low-Dose Ozone as a Eustress Inducer: Experimental Evidence of the Molecular Mechanisms Accounting for Its Therapeutic Action.Int J Mol Sci. 2024 Nov 25;25(23):12657. doi: 10.3390/ijms252312657. Int J Mol Sci. 2024. PMID: 39684369 Free PMC article. Review.
-
Oral Supplementation of Ozonated Sunflower Oil Augments Plasma Antioxidant and Anti-Inflammatory Abilities with Enhancement of High-Density Lipoproteins Functionality in Rats.Antioxidants (Basel). 2024 Apr 26;13(5):529. doi: 10.3390/antiox13050529. Antioxidants (Basel). 2024. PMID: 38790634 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous