

Instantaneous Generation of Subject-Specific Finite Element Models of the Hip Capsule
- PMID: 38247914
- PMCID: PMC10813259
- DOI: 10.3390/bioengineering11010037
Instantaneous Generation of Subject-Specific Finite Element Models of the Hip Capsule
Abstract
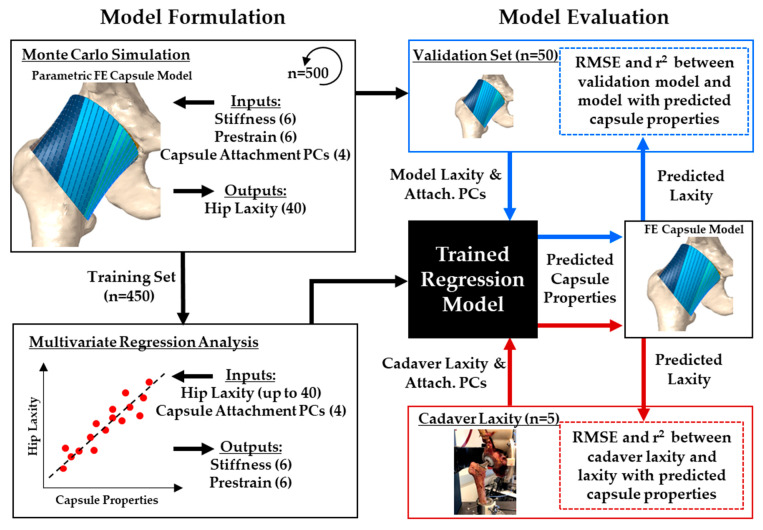
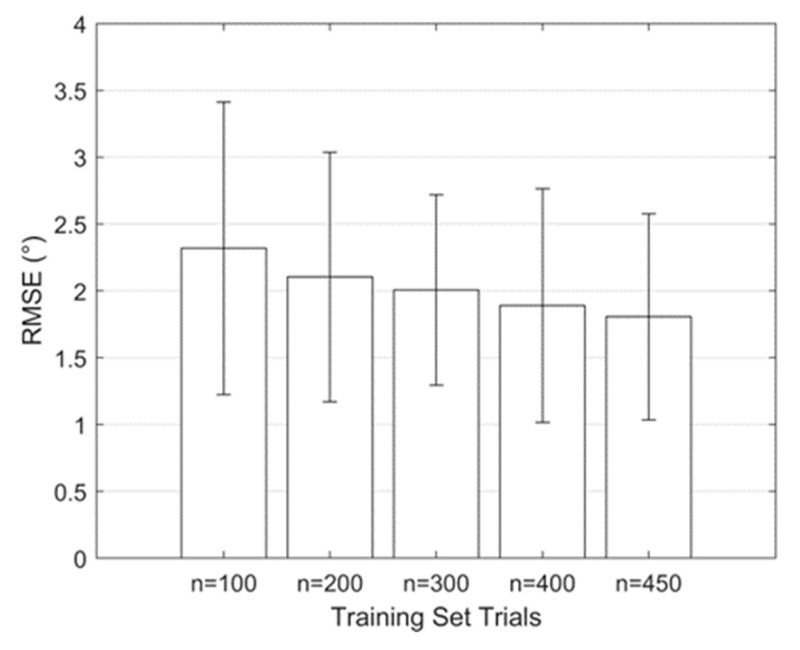
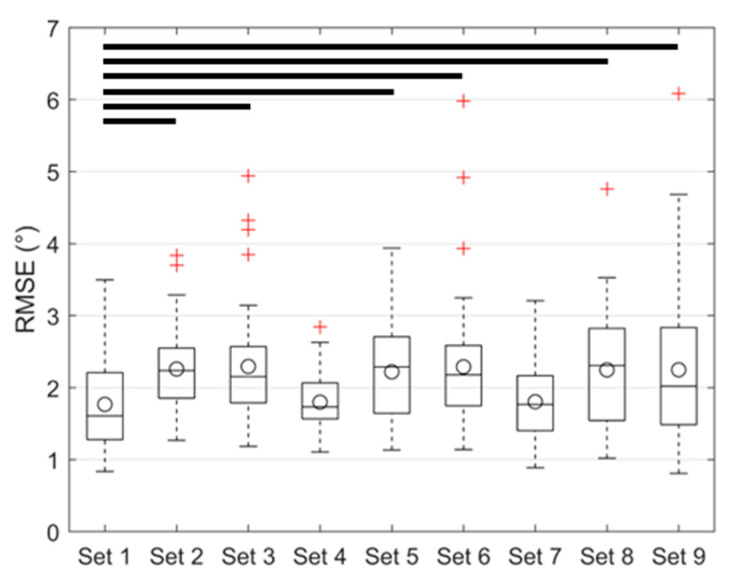
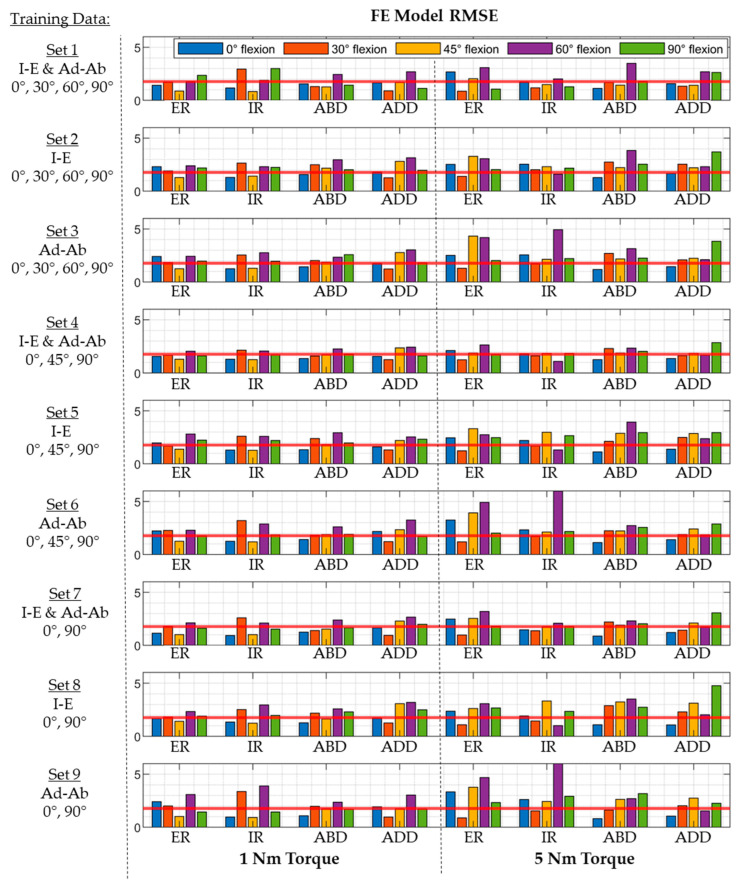
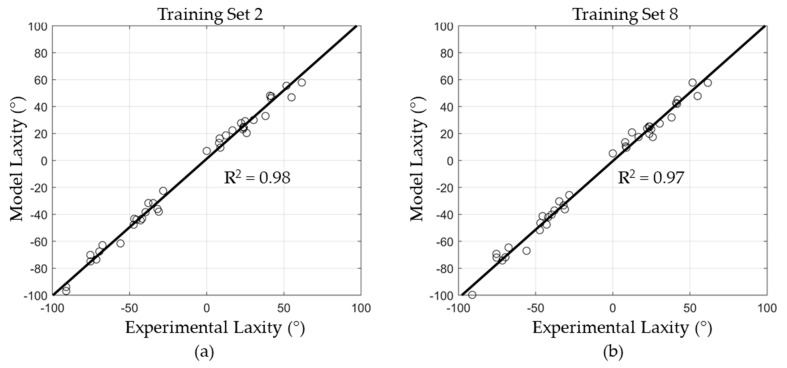
Subject-specific hip capsule models could offer insights into impingement and dislocation risk when coupled with computer-aided surgery, but model calibration is time-consuming using traditional techniques. This study developed a framework for instantaneously generating subject-specific finite element (FE) capsule representations from regression models trained with a probabilistic approach. A validated FE model of the implanted hip capsule was evaluated probabilistically to generate a training dataset relating capsule geometry and material properties to hip laxity. Multivariate regression models were trained using 90% of trials to predict capsule properties based on hip laxity and attachment site information. The regression models were validated using the remaining 10% of the training set by comparing differences in hip laxity between the original trials and the regression-derived capsules. Root mean square errors (RMSEs) in laxity predictions ranged from 1.8° to 2.3°, depending on the type of laxity used in the training set. The RMSE, when predicting the laxity measured from five cadaveric specimens with total hip arthroplasty, was 4.5°. Model generation time was reduced from days to milliseconds. The results demonstrated the potential of regression-based training to instantaneously generate subject-specific FE models and have implications for integrating subject-specific capsule models into surgical planning software.
Keywords: hip capsule; statistical shape model; subject-specific models; surrogate modeling; total hip arthroplasty.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Specimen-specific finite element representations of implanted hip capsules.Comput Methods Biomech Biomed Engin. 2024 May;27(6):751-764. doi: 10.1080/10255842.2023.2200878. Epub 2023 Apr 20. Comput Methods Biomech Biomed Engin. 2024. PMID: 37078790
-
[Prognostic evaluation of hip joint function following capsule repair based on a threedimensional finite element analysis model].Nan Fang Yi Ke Da Xue Xue Bao. 2020 Dec 30;40(12):1826-1830. doi: 10.12122/j.issn.1673-4254.2020.12.20. Nan Fang Yi Ke Da Xue Xue Bao. 2020. PMID: 33380395 Free PMC article. Chinese.
-
Specimen-specific predictions of contact stress under physiological loading in the human hip: validation and sensitivity studies.Biomech Model Mechanobiol. 2014 Apr;13(2):387-400. doi: 10.1007/s10237-013-0504-1. Epub 2013 Jun 5. Biomech Model Mechanobiol. 2014. PMID: 23736783 Free PMC article.
-
The dimensions of the hip capsule can be measured using magnetic resonance imaging and may have a role in arthroscopic planning.Knee Surg Sports Traumatol Arthrosc. 2020 Apr;28(4):1246-1261. doi: 10.1007/s00167-018-5162-5. Epub 2018 Sep 27. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 30259148
-
Hip arthroplasty dislocation risk calculator: evaluation of one million primary implants and twenty-five thousand dislocations with deep learning artificial intelligence in a systematic review of reviews.Int Orthop. 2023 Feb;47(2):557-571. doi: 10.1007/s00264-022-05644-2. Epub 2022 Nov 29. Int Orthop. 2023. PMID: 36445413
Cited by
-
Development of a spinopelvic complex finite element model for quantitative analysis of the biomechanical response of patients with degenerative spondylolisthesis.Med Biol Eng Comput. 2025 Feb;63(2):575-594. doi: 10.1007/s11517-024-03218-5. Epub 2024 Oct 19. Med Biol Eng Comput. 2025. PMID: 39425882
References
LinkOut - more resources
Full Text Sources
