

Intraoperative Laparoscopic Hyperspectral Imaging during Esophagectomy-A Pilot Study Evaluating Esophagogastric Perfusion at the Anastomotic Sites
- PMID: 38247946
- PMCID: PMC10812999
- DOI: 10.3390/bioengineering11010069
Intraoperative Laparoscopic Hyperspectral Imaging during Esophagectomy-A Pilot Study Evaluating Esophagogastric Perfusion at the Anastomotic Sites
Abstract
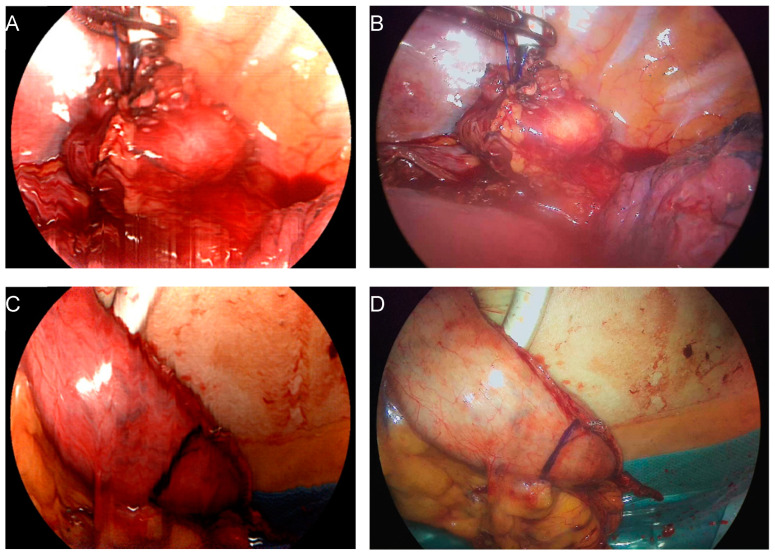
Hyperspectral imaging (HSI) is a non-invasive and contactless technique that enables the real-time acquisition of comprehensive information on tissue within the surgical field. In this pilot study, we investigated whether a new HSI system for minimally-invasive surgery, TIVITA® Mini (HSI-MIS), provides reliable insights into tissue perfusion of the proximal and distal esophagogastric anastomotic sites during 21 laparoscopic/thoracoscopic or robotic Ivor Lewis esophagectomies of patients with cancer to minimize the risk of dreaded anastomotic insufficiency. In this pioneering investigation, physiological tissue parameters were derived from HSI measurements of the proximal site of the anastomosis (esophageal stump) and the distal site of the anastomosis (tip of the gastric conduit) during the thoracic phase of the procedure. Tissue oxygenation (StO2), Near Infrared Perfusion Index (NIR-PI), and Tissue Water Index (TWI) showed similar median values at both anastomotic sites. Significant differences were observed only for NIR-PI (median: 76.5 vs. 63.9; p = 0.012) at the distal site (gastric conduit) compared to our previous study using an HSI system for open surgery. For all 21 patients, reliable and informative measurements were attainable, confirming the feasibility of HSI-MIS to assess anastomotic viability. Further studies on the added benefit of this new technique aiming to reduce anastomotic insufficiency are warranted.
Keywords: clinical evaluation study; esophagectomy; gastrointestinal surgery; hyperspectral imaging; intraoperative imaging; minimally invasive/robotic surgery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





References
-
- Obermannová R., Alsina M., Cervantes A., Leong T., Lordick F., Nilsson M., van Grieken N.C.T., Vogel A., Smyth E.C. Oesophageal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2022;33:992–1004. doi: 10.1016/j.annonc.2022.07.003. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
