

Management of Cytomegalovirus Infections in the Era of the Novel Antiviral Players, Letermovir and Maribavir
- PMID: 38247977
- PMCID: PMC10801527
- DOI: 10.3390/idr16010005
Management of Cytomegalovirus Infections in the Era of the Novel Antiviral Players, Letermovir and Maribavir
Abstract
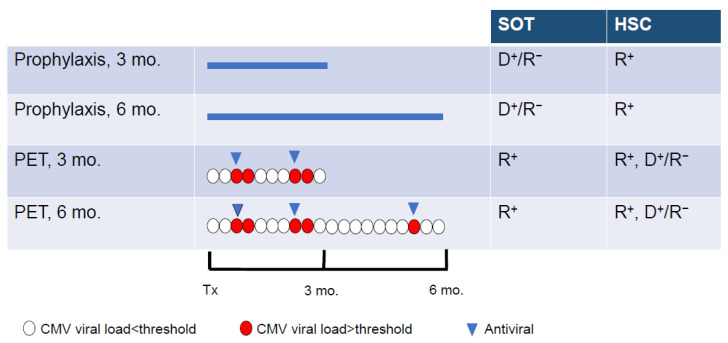
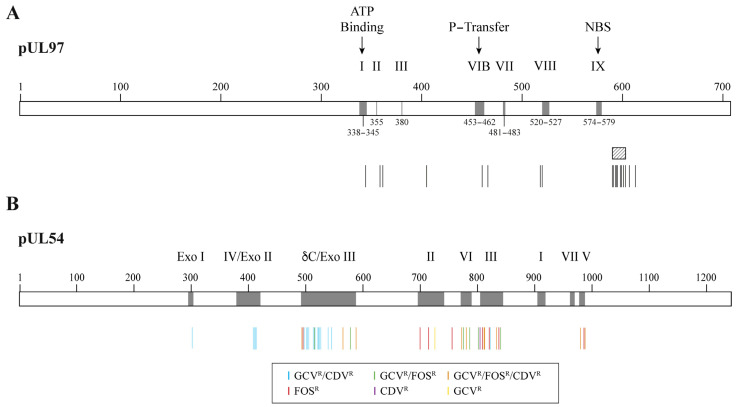
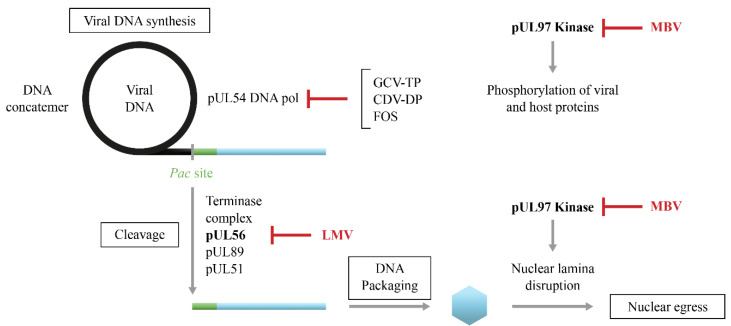
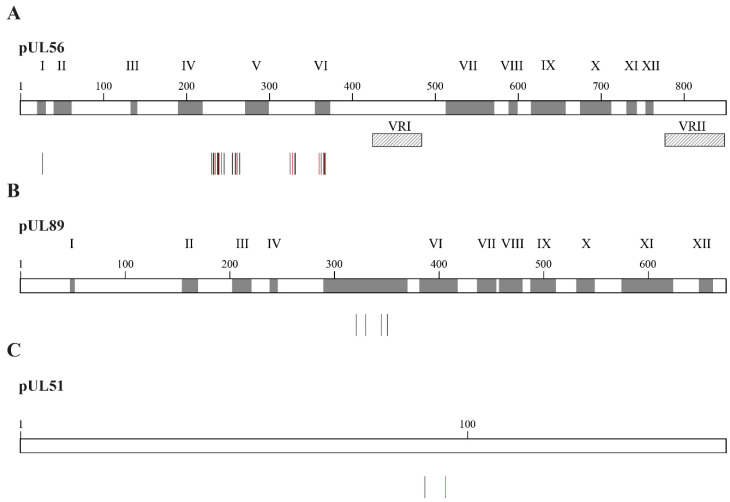
Cytomegalovirus (CMV) infections may increase morbidity and mortality in immunocompromised patients. Until recently, standard antiviral drugs against CMV were limited to viral DNA polymerase inhibitors (val)ganciclovir, foscarnet and cidofovir with a risk for cross-resistance. These drugs may also cause serious side effects. This narrative review provides an update on new antiviral agents that were approved for the prevention and treatment of CMV infections in transplant recipients. Letermovir was approved in 2017 for CMV prophylaxis in CMV-seropositive adults who received an allogeneic hematopoietic stem cell transplant. Maribavir followed four years later, with an indication in the treatment of adult and pediatric transplant patients with refractory/resistant CMV disease. The target of letermovir is the CMV terminase complex (constituted of pUL56, pUL89 and pUL51 subunits). Letermovir prevents the cleavage of viral DNA and its packaging into capsids. Maribavir is a pUL97 kinase inhibitor, which interferes with the assembly of capsids and the egress of virions from the nucleus. Both drugs have activity against most CMV strains resistant to standard drugs and exhibit favorable safety profiles. However, high-level resistance mutations may arise more rapidly in the UL56 gene under letermovir than low-grade resistance mutations. Some mutations emerging in the UL97 gene under maribavir can be cross-resistant with ganciclovir. Thus, letermovir and maribavir now extend the drug arsenal available for the management of CMV infections and their respective niches are currently defined.
Keywords: antiviral drugs; cytomegalovirus; drug resistance; immunocompromised patients; letermovir; maribavir.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Roizman B., Knipe D.M., Whitley R.J. Herpes simplex viruses. In: Knipe D.M., Howley P.M., editors. Fields Virology. 6th ed. Volume 2. Lippincott Williams & Wilkins; Baltimore, MD, USA: 2013. pp. 1823–1897.
-
- Boivin G., Limaye A.P. Goldman-Cecil Medicine. Elsevier; Amsterdam, The Netherlands: 2023. Cytomegalovirus.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
