

Good Performance of Revised Scoring Systems in Predicting Clinical Outcomes of Aeromonas Bacteremia in the Emergency Department: A Retrospective Observational Study
- PMID: 38248001
- PMCID: PMC10814924
- DOI: 10.3390/diagnostics14020124
Good Performance of Revised Scoring Systems in Predicting Clinical Outcomes of Aeromonas Bacteremia in the Emergency Department: A Retrospective Observational Study
Abstract
Background: Aeromonas species, Gram-negative, non-sporulating, facultative, and anaerobic bacilli, widely distributed in aquatic environments, derive various infections, including bacteremia. Most of these infections were opportunistic and found in patients with predisposing conditions. Among the infections, bacteremia remains with notable mortality, reported from 15% to 45%. However, predicting systems for assessing the mortality risk of this disease have yet to be investigated. We aimed to validate the performance of specific predictive scoring systems to assess the clinical outcomes of Aeromonas bacteremia and applied the revised systems to predict mortality risk.
Methods: A retrospective observational study reviewed patients with bacteremia caused by Aeromonas spp. based on at least one positive blood culture sample collected in the emergency department from January 2012 to December 2020. The outcome was in-hospital mortality. We used seven predictive scoring systems to predict the clinical outcome. According to the effectiveness in predicting mortality, we revised three of the seven predictive scoring systems by specific characteristics to refine their risk-predicting performances.
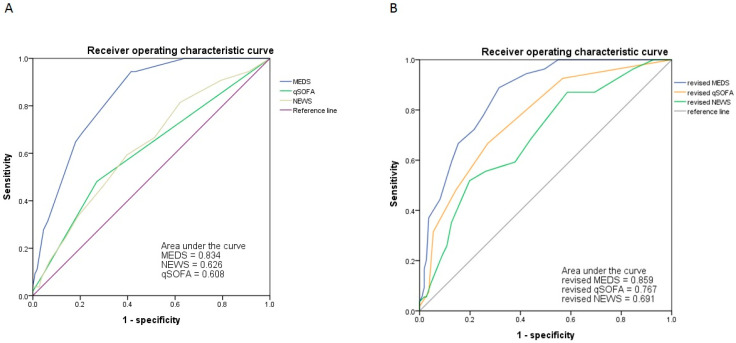
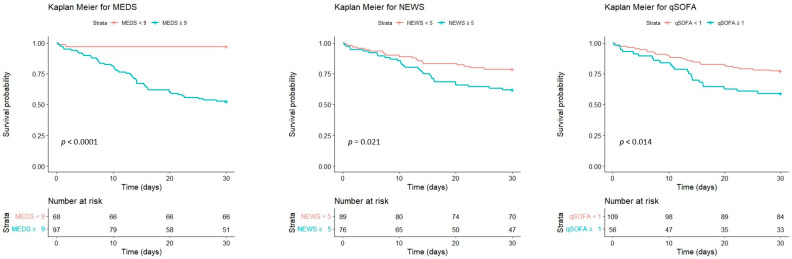
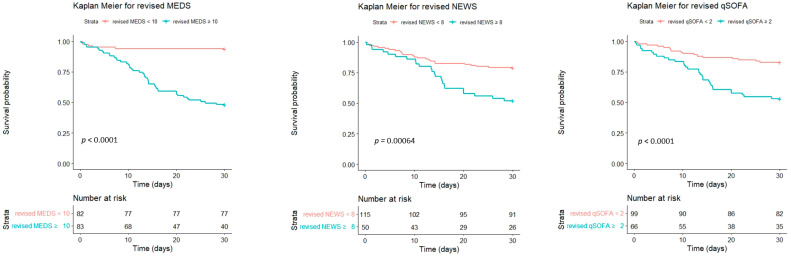
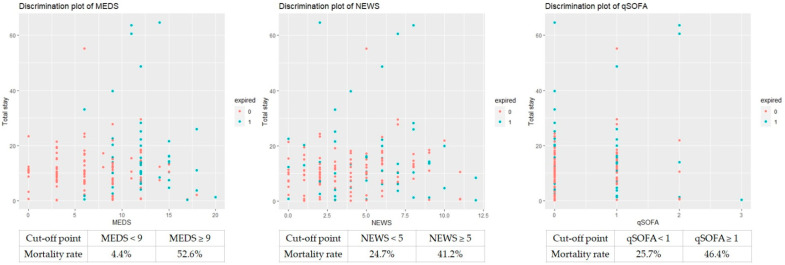
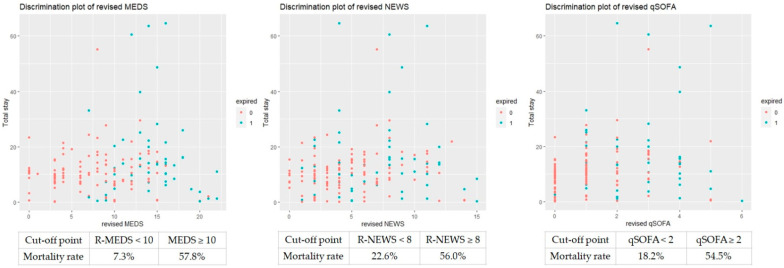
Results: We enrolled 165 patients with bacteremia caused by Aeromonas spp., including 121 males (73.3%) and 44 females (26.7%), with a mean age of 66.1 ± 14.9 years and an average length of hospital stay of 12.4 ± 10.9 days. The overall mortality rate was 32.7% (54/165). The non-survivors had significantly higher scores in MEDS (6.7 ± 4.2 vs. 12.2 ± 3.3, p < 0.001), NEWS (4.0 ± 2.8 vs. 5.3 ± 3.0, p = 0.008), and qSOFA (0.3 ± 0.6 vs. 0.6 ± 0.7, p = 0.007). Regarding mortality risk prediction, the MEDS demonstrated the best predictive power with AUC of ROC measured up to 0.834, followed by NEWS (0.626) and qSOFA (0.608). We revised the MEDS, NEWS, and qSOFA by hemoglobin and lactate. We found that the revised scores had better powerful performance, including 0.859, 0.767, and 0.691 of the AUC of ROC, if the revised MEDS ≥10, revised NEWS ≥8, and revised qSOFA ≥2, respectively.
Conclusions: MEDS, NEWS, and qSOFA were good tools for predicting outcomes in patients with Aeromonas spp. bacteremia. The revised MEDS, NEWS, and qSOFA demonstrated more powerful predicting performance than the original scoring systems. We suggested that patients with higher scores in revised MEDS (≥10), revised NEWS (≥8), and revised qSOFA (≥2) received early goal-directed therapy and appropriate broad-spectrum antibiotic treatment as early as possible to reduce mortality.
Keywords: Aeromonas; bacteremia; mortality risk; scoring systems; temperature.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Risk Factors and Scoring Systems to Predict the Mortality Risk of Afebrile Adult Patients with Monomicrobial Gram-Negative Bacteremia: A 10-Year Observational Study in the Emergency Department.Diagnostics (Basel). 2024 Apr 23;14(9):869. doi: 10.3390/diagnostics14090869. Diagnostics (Basel). 2024. PMID: 38732284 Free PMC article.
-
Better Performance of Modified Scoring Systems to Predict the Clinical Outcomes of Vibrio Bacteremia in the Emergency Department: An Observational Study.J Pers Med. 2024 Apr 3;14(4):385. doi: 10.3390/jpm14040385. J Pers Med. 2024. PMID: 38673012 Free PMC article.
-
Performance of Scoring Systems in Predicting Clinical Outcomes in Patients with Bacteremia of Listeria monocytogenes: A 9-Year Hospital-Based Study.Biology (Basel). 2021 Oct 21;10(11):1073. doi: 10.3390/biology10111073. Biology (Basel). 2021. PMID: 34827066 Free PMC article.
-
Comparison of qSOFA and Hospital Early Warning Scores for prognosis in suspected sepsis in emergency department patients: a systematic review.Emerg Med J. 2022 Apr;39(4):284-294. doi: 10.1136/emermed-2020-210416. Epub 2021 Aug 17. Emerg Med J. 2022. PMID: 34404680
-
Performance of the MEDS score in predicting mortality among emergency department patients with a suspected infection: a meta-analysis.Emerg Med J. 2020 Apr;37(4):232-239. doi: 10.1136/emermed-2019-208901. Epub 2019 Dec 13. Emerg Med J. 2020. PMID: 31836584
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
