

Imaging Features of Plantar Vein Thrombosis: An Easily Overlooked Condition in the Differential Diagnosis of Foot Pain
- PMID: 38248003
- PMCID: PMC10814699
- DOI: 10.3390/diagnostics14020126
Imaging Features of Plantar Vein Thrombosis: An Easily Overlooked Condition in the Differential Diagnosis of Foot Pain
Abstract
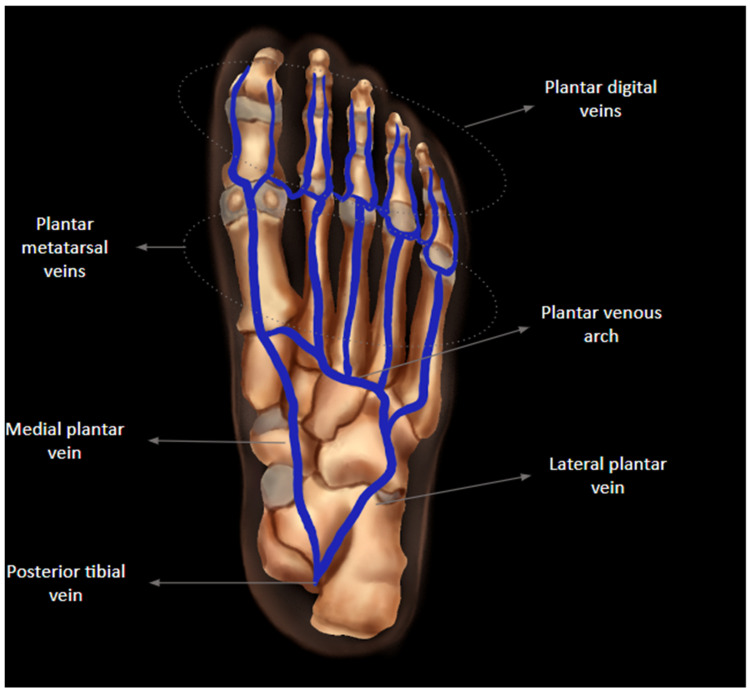
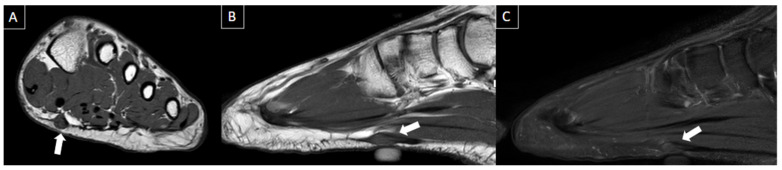
Plantar vein thrombosis is a venous disorder affecting deep plantar veins that can manifest with non-specific localized pain, plantar foot pain, swelling, and sensation of fullness. Plantar veins are not routinely assessed during sonographic scans for deep venous thrombosis, which makes plantar venous thrombosis a commonly missed diagnosis. This paper provides a comprehensive review of the venous anatomy of the foot and imaging findings of plantar venous thrombosis as well as discusses the current literature on the topic and its differential diagnoses.
Keywords: DVT; Doppler; MRI; deep venous thrombosis; foot pain; metatarsalgia; thrombophlebitis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
















Similar articles
-
Magnetic Resonance Imaging Features of Plantar Vein Thrombosis.Diagnostics (Basel). 2024 Jun 8;14(12):1215. doi: 10.3390/diagnostics14121215. Diagnostics (Basel). 2024. PMID: 38928631 Free PMC article.
-
Plantar vein thrombosis.Phlebology. 2021 Feb;36(1):26-31. doi: 10.1177/0268355520946620. Epub 2020 Jul 28. Phlebology. 2021. PMID: 32722984
-
Clinical characteristics and course of plantar vein thrombosis: a series of 22 cases.Phlebology. 2015 Dec;30(10):714-8. doi: 10.1177/0268355514555385. Epub 2014 Oct 17. Phlebology. 2015. PMID: 25326214
-
Sonographic diagnosis of clinically unsuspected thrombosis of the medial marginal vein and dorsal arch of the foot.J Ultrasound. 2021 Dec;24(4):515-518. doi: 10.1007/s40477-019-00421-1. Epub 2020 Jan 9. J Ultrasound. 2021. PMID: 31919813 Free PMC article. Review.
-
Spontaneous plantar vein thrombosis: state of the art.Phlebology. 2013 Dec;28(8):432-7. doi: 10.1177/0268355513477087. Epub 2013 May 6. Phlebology. 2013. PMID: 23520215 Review.
Cited by
-
Diagnosis of plantar vein thrombosis by vascular ultrasound: a case report.J Vasc Bras. 2025 Jun 16;24:e20240081. doi: 10.1590/1677-5449.202400812. eCollection 2025. J Vasc Bras. 2025. PMID: 40557049 Free PMC article.
-
Radiological approach to metatarsalgia in current practice: an educational review.Insights Imaging. 2025 Apr 29;16(1):94. doi: 10.1186/s13244-025-01945-3. Insights Imaging. 2025. PMID: 40301191 Free PMC article.
-
Magnetic Resonance Imaging Features of Plantar Vein Thrombosis.Diagnostics (Basel). 2024 Jun 8;14(12):1215. doi: 10.3390/diagnostics14121215. Diagnostics (Basel). 2024. PMID: 38928631 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
