

Contemporary Evidence and Practice on Right Heart Catheterization in Patients with Acute or Chronic Heart Failure
- PMID: 38248013
- PMCID: PMC10814482
- DOI: 10.3390/diagnostics14020136
Contemporary Evidence and Practice on Right Heart Catheterization in Patients with Acute or Chronic Heart Failure
Abstract
Heart failure (HF) has a global prevalence of 1-2%, and the incidence around the world is growing. The prevalence increases with age, from around 1% for those aged <55 years to >10% for those aged 70 years or over. Based on studies in hospitalized patients, about 50% of patients have heart failure with reduced ejection fraction (HFrEF), and 50% have heart failure with preserved ejection fraction (HFpEF). HF is associated with high morbidity and mortality, and HF-related hospitalizations are common, costly, and impact both quality of life and prognosis. More than 5-10% of patients deteriorate into advanced HF (AdHF) with worse outcomes, up to cardiogenic shock (CS) condition. Right heart catheterization (RHC) is essential to assess hemodynamics in the diagnosis and care of patients with HF. The aim of this article is to review the evidence on RHC in various clinical scenarios of patients with HF.
Keywords: HFpEF; HFrEF; acute heart failure; advanced heart failure; cardiogenic shock; chronic heart failure; heart failure; right heart catheterization.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Binanay C., Califf R.M., Hasselblad V., O’Connor C.M., Shah M.R., Sopko G., Stevenson L.W., Francis G.S., Leier C.V., Miller L.W., et al. Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness: The ESCAPE Trial. JAMA. 2005;294:1625–1633. doi: 10.1001/jama.294.13.1625. - DOI - PubMed
-
- Kittleson M.M., Panjrath G.S., Amancherla K., Davis L.L., Deswal A., Dixon D.L., Januzzi J.L., Yancy C.W. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure with Preserved Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2023;81:1835–1878. doi: 10.1016/j.jacc.2023.03.393. - DOI - PubMed
-
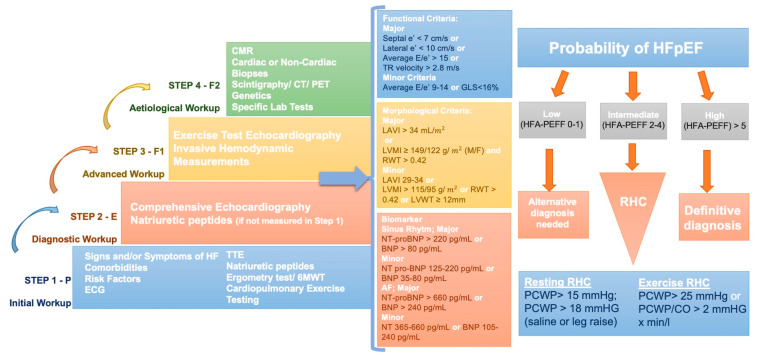
- Pieske B., Tschöpe C., de Boer R.A., Fraser A.G., Anker S.D., Donal E., Edelmann F., Fu M., Guazzi M., Lam C.S.P., et al. How to Diagnose Heart Failure with Preserved Ejection Fraction: The HFA-PEFF Diagnostic Algorithm: A Consensus Recommendation from the Heart Failure Association (HFA) of the European Society of Cardiology (ESC) Eur. Heart J. 2019;40:3297–3317. doi: 10.1093/eurheartj/ehz641. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
