

Predictive Factors Correlated with Successful Early Endoscopic Removal of Pancreaticolithiasis in Chronic Pancreatitis after Extracorporeal Shock Wave Lithotripsy
- PMID: 38248049
- PMCID: PMC10814896
- DOI: 10.3390/diagnostics14020172
Predictive Factors Correlated with Successful Early Endoscopic Removal of Pancreaticolithiasis in Chronic Pancreatitis after Extracorporeal Shock Wave Lithotripsy
Abstract
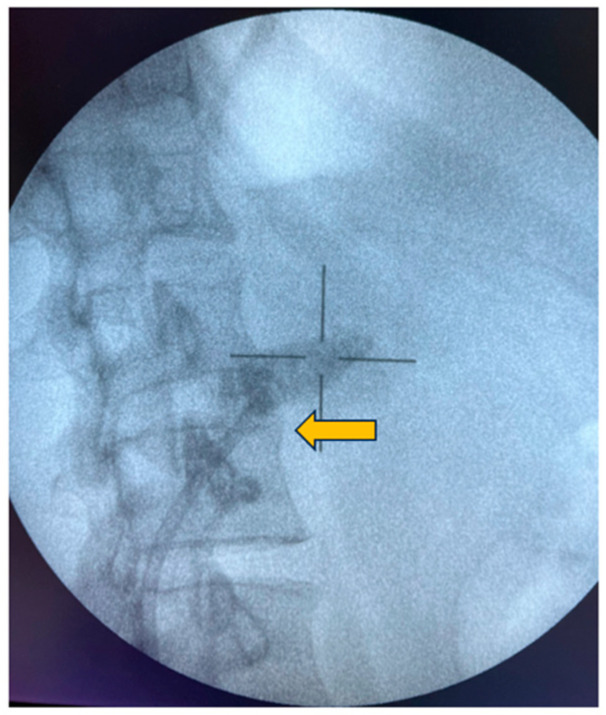
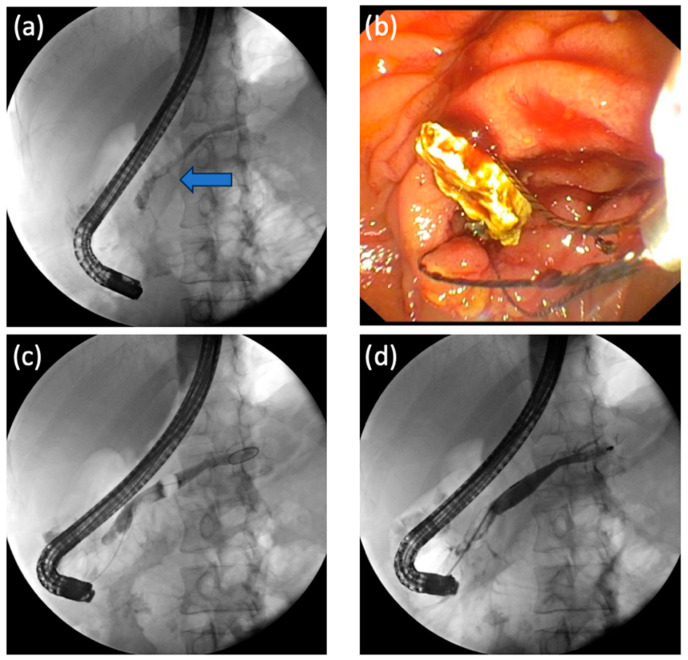
Background: The treatment of chronic pancreatitis (CP) and symptomatic pancreatic duct (PD) calculi often involves techniques like endoscopic retrograde cholangiopancreatography (ERCP), extracorporeal shock wave lithotripsy (ESWL), or a combination of both. However, identifying predictive factors for the successful removal of these calculi remains variable. This study aimed to determine the factors predicting successful ESWL and endoscopic removal in CP and PD calculi patients.
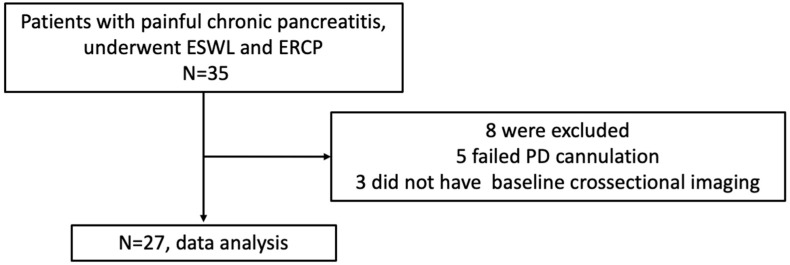
Methods: We examined data from CP patients who underwent complete PD calculi removal via ESWL combined with ERCP between July 2012 and 2022, and assessed baseline characteristics, imaging findings, and treatment details. Patients were categorized into early- and late-endoscopic complete removal groups (EER and LER groups, respectively).
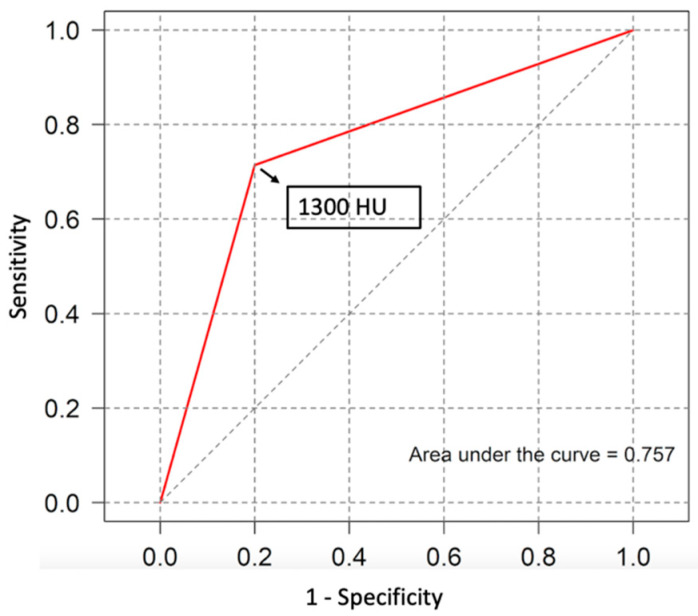
Results: Of the 27 patients analyzed, 74.1% were male with an average age of 44 ± 9.6 years. EER was achieved in 74% of the patients. Patients in the EER group exhibited smaller PD calculi diameter (8.5 vs. 19 mm, p = 0.012) and lower calculus density (964.6 vs. 1313.3 HU, p = 0.041) compared to the LER group. Notably, PD stricture and the rate of PD stent insertion were not different between the groups. A calculus density threshold of 1300 HU on non-contrast CT demonstrated 71% sensitivity and 80% specificity in predicting EER.
Conclusions: Smaller and low-density PD calculi may serve as predictors for successful EER, potentially aiding in the management of CP patients with PD calculi.
Keywords: Pancreaticolithiasis; chronic pancreatitis; endoscopic clearance; endoscopic retrograde cholangiopancreatography; extracorporeal shockwave lithotripsy; pancreatic calculi; pancreatic stone density; predictive factors.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Timing of ERCP after extracorporeal shock wave lithotripsy for large main pancreatic duct stones.Surg Endosc. 2023 Dec;37(12):9098-9104. doi: 10.1007/s00464-023-10467-2. Epub 2023 Oct 5. Surg Endosc. 2023. PMID: 37798530
-
Duct Diameter and Size of Stones Predict Successful Extracorporeal Shock Wave Lithotripsy and Endoscopic Clearance in Patients With Chronic Pancreatitis and Pancreaticolithiasis.Pancreas. 2016 Sep;45(8):1208-11. doi: 10.1097/MPA.0000000000000622. Pancreas. 2016. PMID: 26967455
-
Extracorporeal shock wave lithotripsy for prevention of recurrent pancreatitis caused by obstructive pancreatic stones.Pancreas. 2010 Mar;39(2):153-5. doi: 10.1097/MPA.0b013e3181bb1733. Pancreas. 2010. PMID: 19820418
-
Multiple main pancreatic duct stones in tropical pancreatitis: safe clearance with extracorporeal shockwave lithotripsy.J Gastroenterol Hepatol. 2006 Oct;21(10):1514-8. doi: 10.1111/j.1440-1746.2006.04224.x. J Gastroenterol Hepatol. 2006. PMID: 16928210 Review.
-
The role of extracorporeal shock wave lithotripsy in the treatment of chronic pancreatitis.Acta Gastroenterol Belg. 2021 Oct-Dec;84(4):620-626. doi: 10.51821/84.4.027. Acta Gastroenterol Belg. 2021. PMID: 34965044 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
