

Rejection Requiring Treatment within the First Year following Heart Transplantation: The UNOS Insight
- PMID: 38248753
- PMCID: PMC10817284
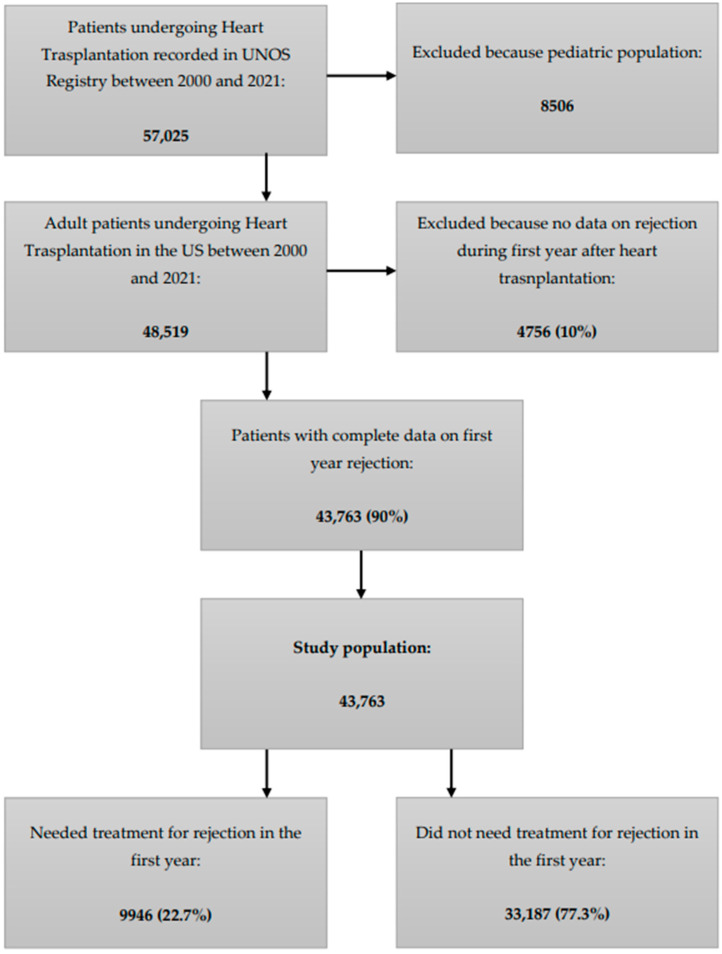
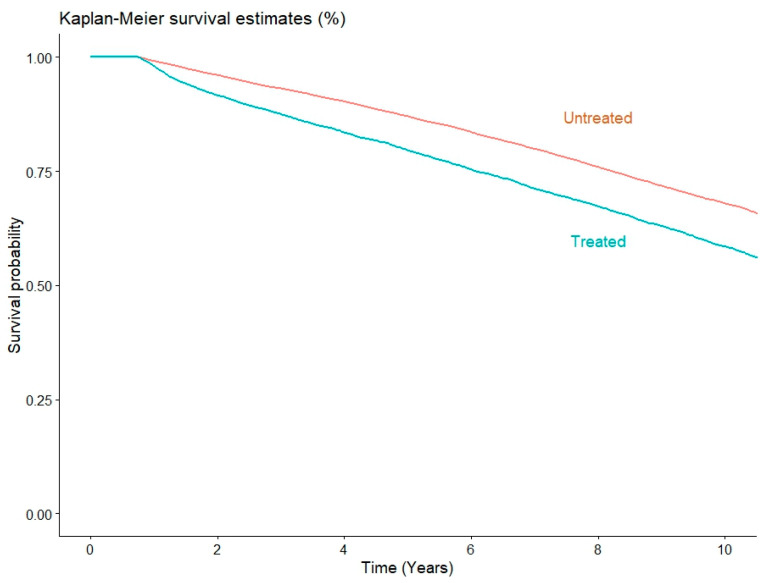
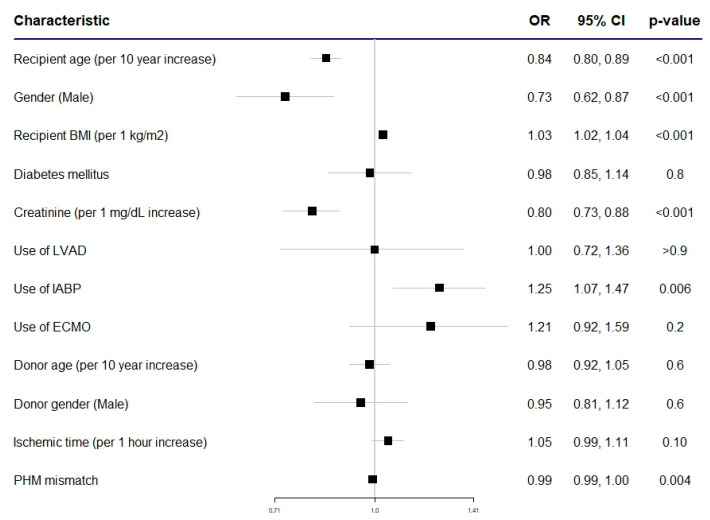
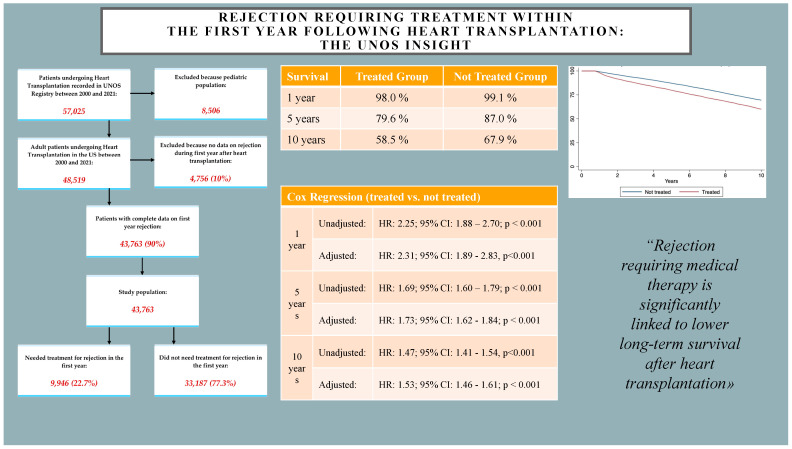
- DOI: 10.3390/jpm14010052
Rejection Requiring Treatment within the First Year following Heart Transplantation: The UNOS Insight
Abstract
(1) Background: Heart failure is an extremely impactful health issue from both a social and quality-of-life point of view and the rate of patients with this condition is destined to rise in the next few years. Transplantation remains the mainstay of treatment for end-stage heart failure, but a shortage of organs represents a significant problem that prolongs time spent on the waiting list. In view of this, the selection of donor and recipient must be extremely meticulous, considering all factors that could predispose to organ failure. One of the main considerations regarding heart transplants is the risk of graft rejection and the need for immunosuppression therapy to mitigate that risk. In this study, we aimed to assess the characteristics of patients who need immunosuppression treatment for rejection within one year of heart transplantation and its impact on mid-term and long-term mortality. (2) Methods: The United Network for Organ Sharing (UNOS) Registry was queried to identify patients who solely underwent a heart transplant in the US between 2000 and 2021. Patients were divided into two groups according to the need for anti-rejection treatment within one year of heart transplantation. Patients' characteristics in the two groups were assessed, and 1 year and 10 year mortality rates were compared. (3) Results: A total of 43,763 patients underwent isolated heart transplantation in the study period, and 9946 (22.7%) needed anti-rejection treatment in the first year. Patients who required treatment for rejection within one year after transplant were more frequently younger (49 ± 14 vs. 52 ± 14 years, p < 0.001), women (31% vs. 23%, p < 0.001), and had a higher CPRA value (14 ± 26 vs. 11 ± 23, p < 0.001). Also, the rate of prior cardiac surgery was more than double in this group (27% vs. 12%, p < 0.001), while prior LVAD (12% vs. 11%, p < 0.001) and IABP (10% vs. 9%, p < 0.01) were more frequent in patients who did not receive anti-rejection treatment in the first year. Finally, pre-transplantation creatinine was significantly higher in patients who did not need treatment for rejection in the first year (1.4 vs. 1.3, p < 0.01). Most patients who did not require anti-rejection treatment underwent heart transplantation during the new allocation era, while less than half of the patients who required treatment underwent transplantation after the new allocation policy implementation (65% vs. 49%, p < 0.001). Patients who needed rejection treatment in the first year had a higher risk of unadjusted 1 year (HR: 2.25; 95% CI: 1.88-2.70; p < 0.001), 5 year (HR: 1.69; 95% CI: 1.60-1.79; p < 0.001), and 10 year (HR: 1.47; 95% CI: 1.41-1.54, p < 0.001) mortality, and this was confirmed at the adjusted analysis at all three time-points. (4) Conclusions: Medical treatment of acute rejection was associated with significantly increased 1 year mortality compared to patients who did not require anti-rejection therapy. The higher risk of mortality was confirmed at a 10 year follow-up. Further studies and newer follow-up data are required to investigate the role of anti-rejection therapy in the heart transplant population.
Keywords: UNOS Registry; heart transplantation; long-term outcomes; personalized immunosuppression.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., Anderson C.A.M., Arora P., Avery C.L., Baker-Smith C.M., Beaton A.Z., Boehme A.K., Buxton A.E., et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation. 2023;147:e93–e621. doi: 10.1161/CIR.0000000000001123. - DOI - PubMed
-
- Kalogeropoulos A.P., Samman-Tahhan A., Hedley J.S., McCue A.A., Bjork J.B., Markham D.W., Bhatt K.N., Georgiopoulou V.V., Smith A.L., Butler J. Progression to Stage D Heart Failure Among Outpatients with Stage C Heart Failure and Reduced Ejection Fraction. JACC Heart Fail. 2017;5:528–537. doi: 10.1016/j.jchf.2017.02.020. - DOI - PubMed
LinkOut - more resources
Full Text Sources
