

Obesity, Dietary Fats, and Gastrointestinal Cancer Risk-Potential Mechanisms Relating to Lipid Metabolism and Inflammation
- PMID: 38248845
- PMCID: PMC10821017
- DOI: 10.3390/metabo14010042
Obesity, Dietary Fats, and Gastrointestinal Cancer Risk-Potential Mechanisms Relating to Lipid Metabolism and Inflammation
Abstract
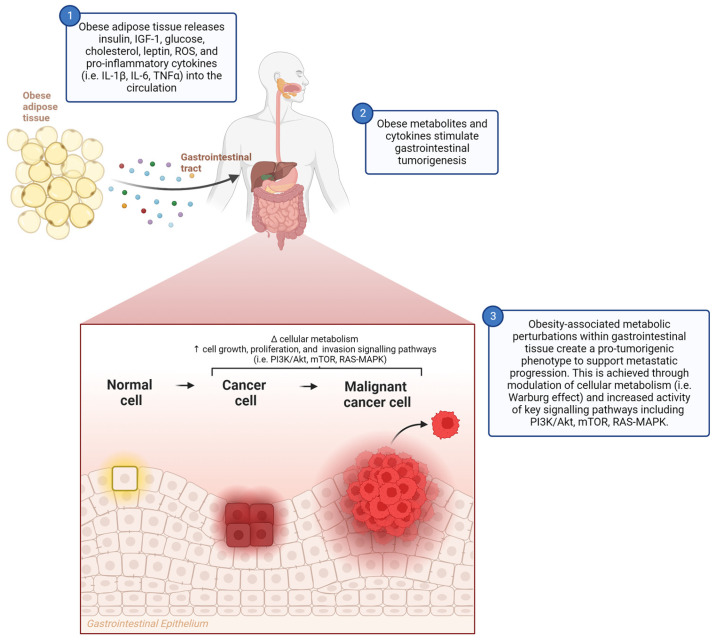
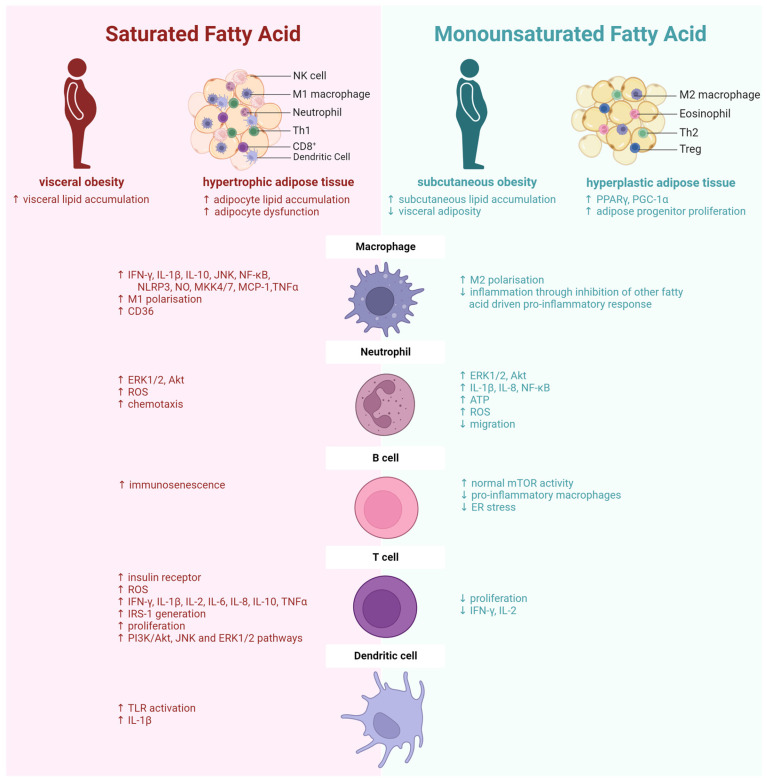
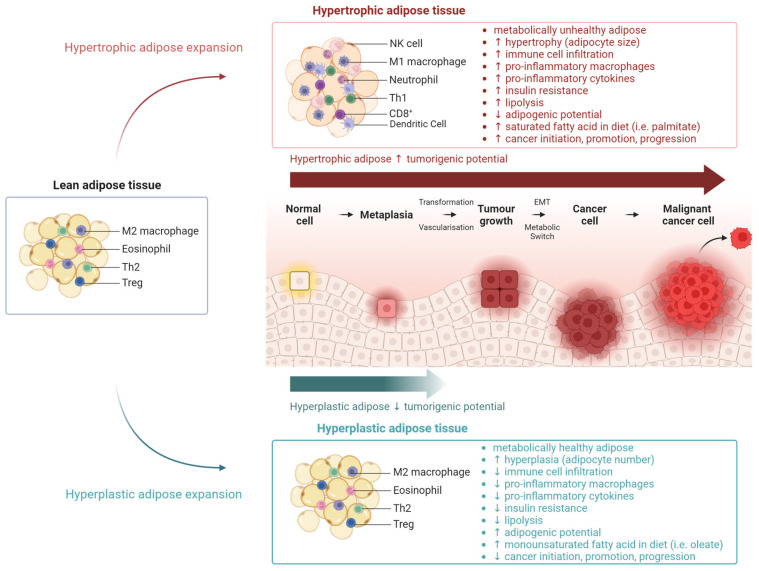
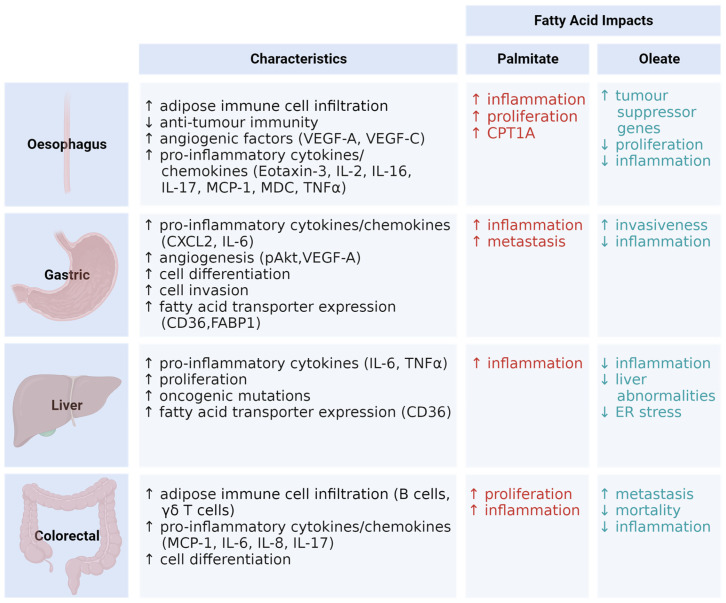
Obesity is a major driving factor in the incidence, progression, and poor treatment response in gastrointestinal cancers. Herein, we conducted a comprehensive analysis of the impact of obesity and its resulting metabolic perturbations across four gastrointestinal cancer types, namely, oesophageal, gastric, liver, and colorectal cancer. Importantly, not all obese phenotypes are equal. Obese adipose tissue heterogeneity depends on the location, structure, cellular profile (including resident immune cell populations), and dietary fatty acid intake. We discuss whether adipose heterogeneity impacts the tumorigenic environment. Dietary fat quality, in particular saturated fatty acids, promotes a hypertrophic, pro-inflammatory adipose profile, in contrast to monounsaturated fatty acids, resulting in a hyperplastic, less inflammatory adipose phenotype. The purpose of this review is to examine the impact of obesity, including dietary fat quality, on adipose tissue biology and oncogenesis, specifically focusing on lipid metabolism and inflammatory mechanisms. This is achieved with a particular focus on gastrointestinal cancers as exemplar models of obesity-associated cancers.
Keywords: adipose; diet; gastrointestinal cancer; inflammation; metabolism; monounsaturated fatty acids; obesity; saturated fatty acids.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Site-specific differences in the fatty acid composition of abdominal adipose tissue in an obese population from a Mediterranean area: relation with dietary fatty acids, plasma lipid profile, serum insulin, and central obesity.Am J Clin Nutr. 2001 Nov;74(5):585-91. doi: 10.1093/ajcn/74.5.585. Am J Clin Nutr. 2001. PMID: 11684525
-
Dietary habits affect fatty acid composition of visceral adipose tissue in subjects with colorectal cancer or obesity.Eur J Nutr. 2020 Jun;59(4):1463-1472. doi: 10.1007/s00394-019-02003-7. Epub 2019 May 22. Eur J Nutr. 2020. PMID: 31119400
-
Dietary Fat and Cancer-Which Is Good, Which Is Bad, and the Body of Evidence.Int J Mol Sci. 2020 Jun 9;21(11):4114. doi: 10.3390/ijms21114114. Int J Mol Sci. 2020. PMID: 32526973 Free PMC article. Review.
-
Diets high in monounsaturated and polyunsaturated fatty acids decrease fatty acid synthase protein levels in adipose tissue but do not alter other markers of adipose function and inflammation in diet-induced obese rats.Prostaglandins Leukot Essent Fatty Acids. 2014 Feb-Mar;90(2-3):77-84. doi: 10.1016/j.plefa.2013.12.002. Epub 2013 Dec 12. Prostaglandins Leukot Essent Fatty Acids. 2014. PMID: 24411719
-
Dietary lipids in early development: relevance to obesity, immune and inflammatory disorders.Curr Opin Endocrinol Diabetes Obes. 2007 Oct;14(5):359-64. doi: 10.1097/MED.0b013e3282be90b9. Curr Opin Endocrinol Diabetes Obes. 2007. PMID: 17940463 Review.
Cited by
-
Non-Specific Elevated Serum Free Fatty Acids in Lung Cancer Patients: Nutritional or Pathological?Nutrients. 2024 Aug 28;16(17):2884. doi: 10.3390/nu16172884. Nutrients. 2024. PMID: 39275200 Free PMC article.
-
Relationship between obesity indexes and triglyceride glucose index with gastrointestinal cancer among the US population.Prev Med Rep. 2024 May 17;43:102760. doi: 10.1016/j.pmedr.2024.102760. eCollection 2024 Jul. Prev Med Rep. 2024. PMID: 38818028 Free PMC article.
-
Gene and lncRNA Profiling of ω3/ω6 Polyunsaturated Fatty Acid-Exposed Human Visceral Adipocytes Uncovers Different Responses in Healthy Lean, Obese and Colorectal Cancer-Affected Individuals.Int J Mol Sci. 2024 Mar 15;25(6):3357. doi: 10.3390/ijms25063357. Int J Mol Sci. 2024. PMID: 38542331 Free PMC article.
-
Anoikis resistance in gastric cancer: a comprehensive review.Cell Death Dis. 2025 Jul 15;16(1):528. doi: 10.1038/s41419-025-07860-1. Cell Death Dis. 2025. PMID: 40664635 Free PMC article. Review.
-
Mechanisms underlying obesity-malignancy connection: a systematic narrative review.J Physiol Biochem. 2025 May;81(2):403-439. doi: 10.1007/s13105-025-01084-9. Epub 2025 May 23. J Physiol Biochem. 2025. PMID: 40408050
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
