

Trajectories of Host-Response Subphenotypes in Patients With COVID-19 Across the Spectrum of Respiratory Support
- PMID: 38250011
- PMCID: PMC10798236
- DOI: 10.1016/j.chstcc.2023.100018
Trajectories of Host-Response Subphenotypes in Patients With COVID-19 Across the Spectrum of Respiratory Support
Abstract
Background: Hospitalized patients with severe COVID-19 follow heterogeneous clinical trajectories, requiring different levels of respiratory support and experiencing diverse clinical outcomes. Differences in host immune responses to SARS-CoV-2 infection may account for the heterogeneous clinical course, but we have limited data on the dynamic evolution of systemic biomarkers and related subphenotypes. Improved understanding of the dynamic transitions of host subphenotypes in COVID-19 may allow for improved patient selection for targeted therapies.
Research question: We examined the trajectories of host-response profiles in severe COVID-19 and evaluated their prognostic impact on clinical outcomes.
Study design and methods: In this prospective observational study, we enrolled 323 inpatients with COVID-19 receiving different levels of baseline respiratory support: (1) low-flow oxygen (37%), (2) noninvasive ventilation (NIV) or high-flow oxygen (HFO; 29%), (3) invasive mechanical ventilation (27%), and (4) extracorporeal membrane oxygenation (7%). We collected plasma samples on enrollment and at days 5 and 10 to measure host-response biomarkers. We classified patients by inflammatory subphenotypes using two validated predictive models. We examined clinical, biomarker, and subphenotype trajectories and outcomes during hospitalization.
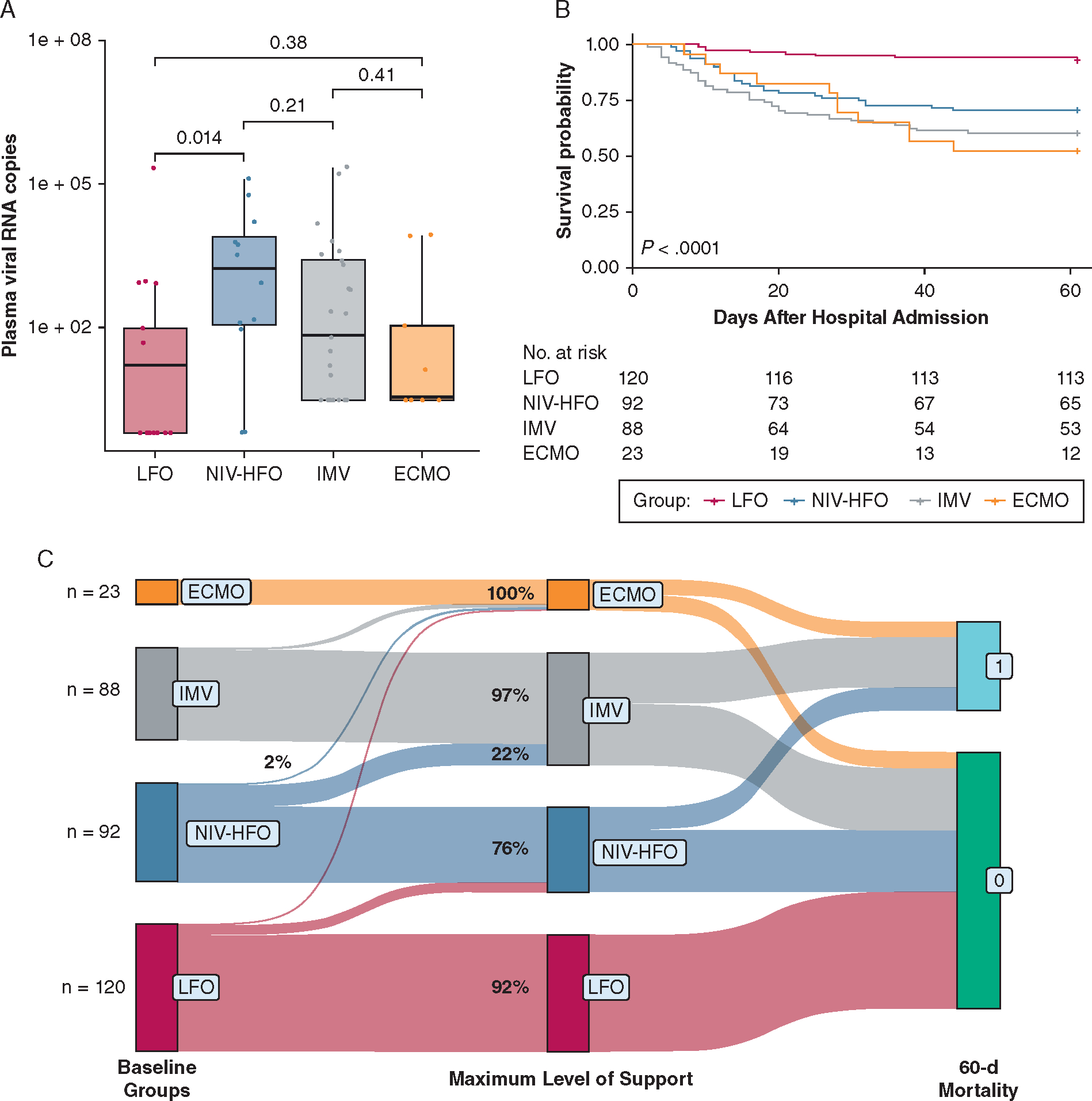
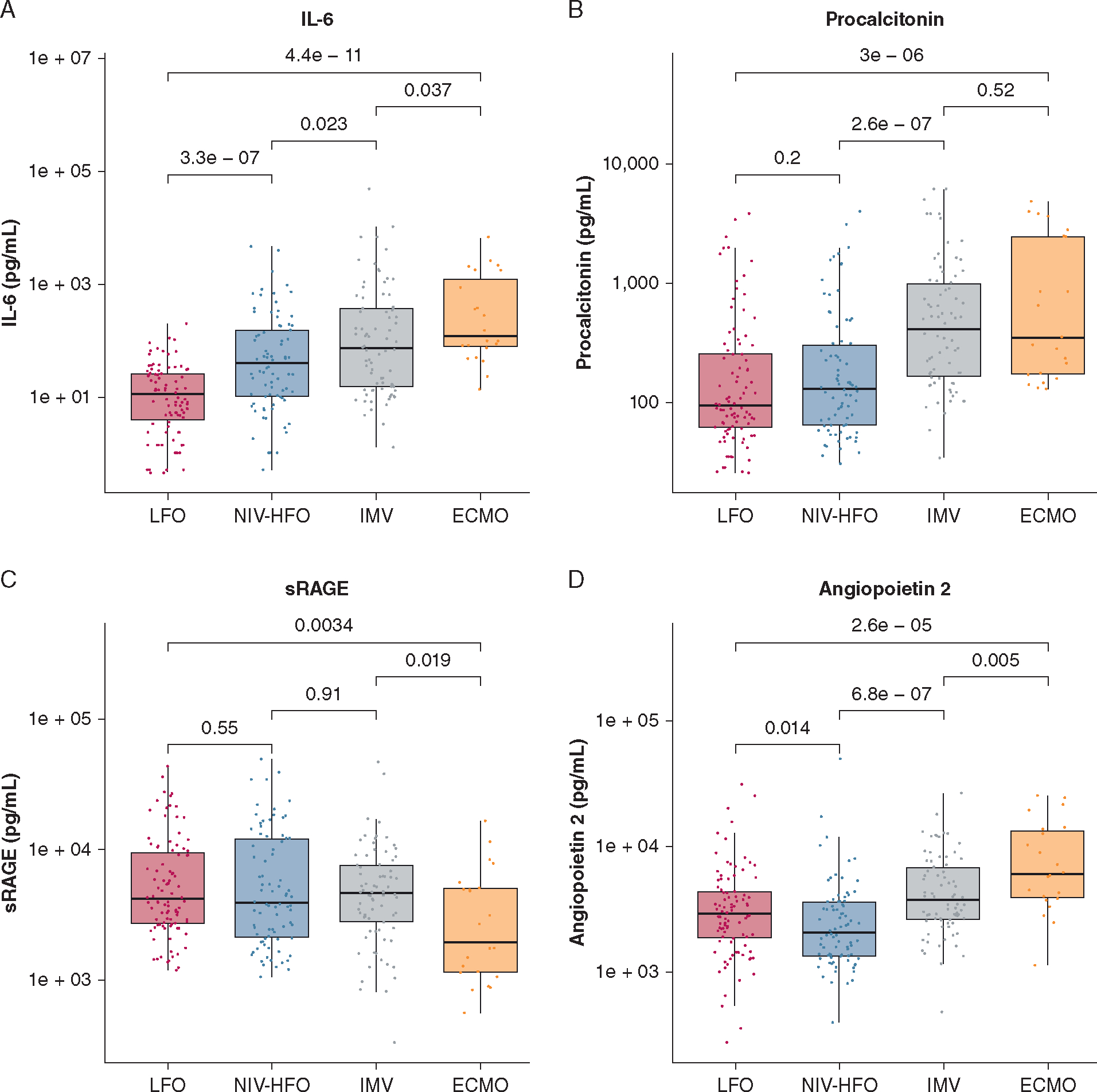
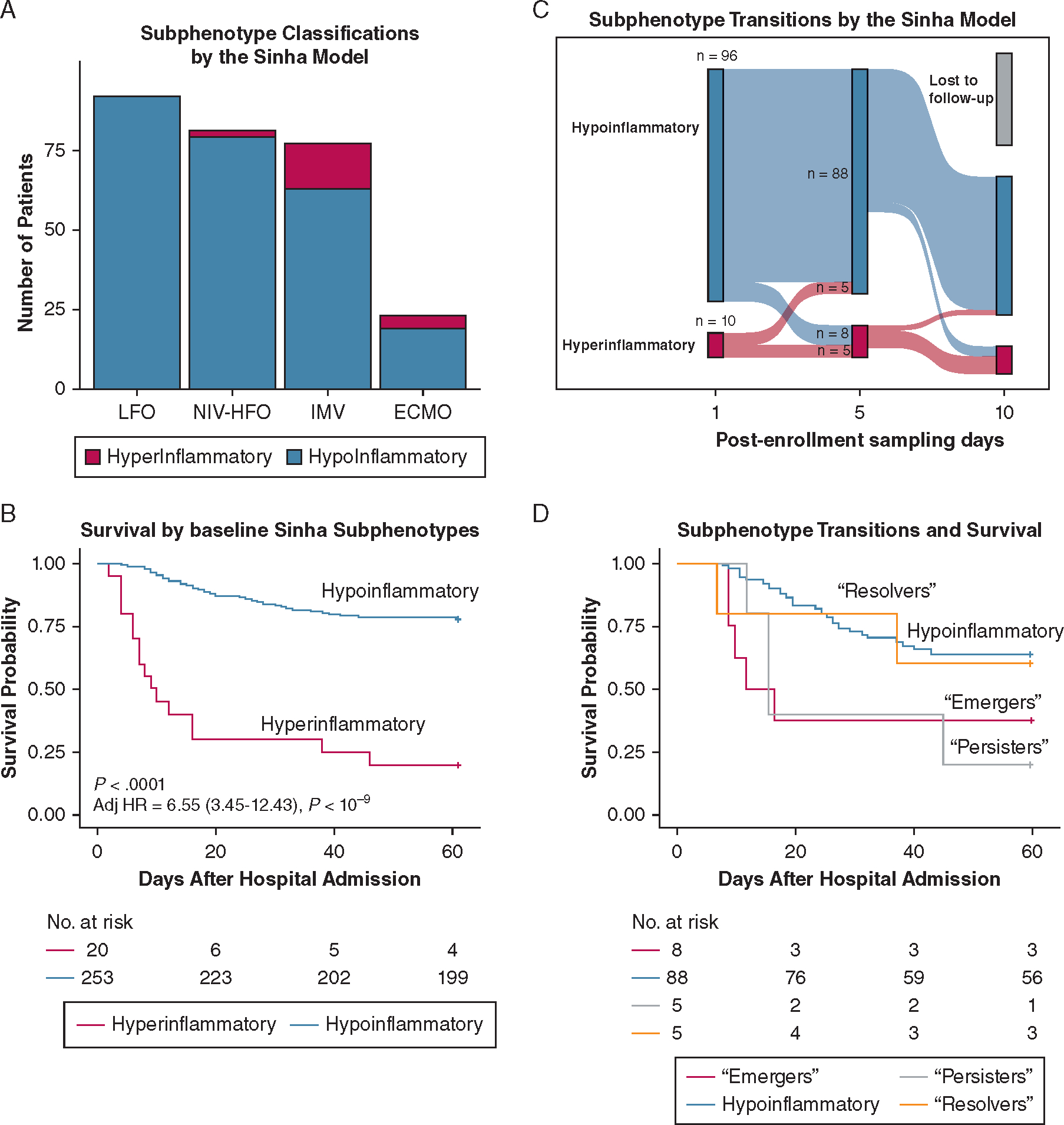
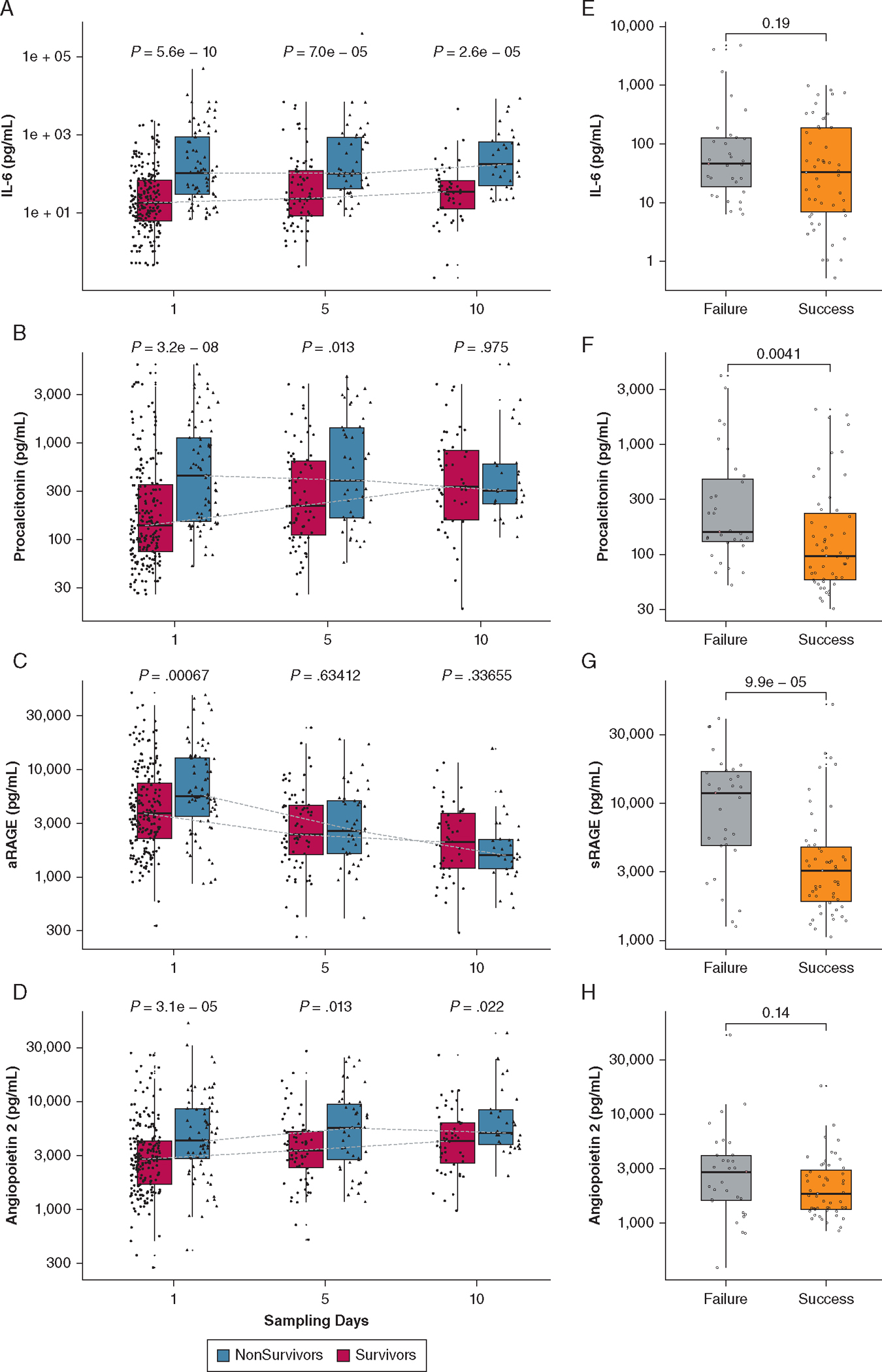
Results: IL-6, procalcitonin, and angiopoietin 2 persistently were elevated in patients receiving higher levels of respiratory support, whereas soluble receptor of advanced glycation end products (sRAGE) levels displayed the inverse pattern. Patients receiving NIV or HFO at baseline showed the most dynamic clinical trajectory, with 24% eventually requiring intubation and exhibiting worse 60-day mortality than patients receiving invasive mechanical ventilation at baseline (67% vs 35%; P < .0001). sRAGE levels predicted NIV failure and worse 60-day mortality for patients receiving NIV or HFO, whereas IL-6 levels were predictive in all patients regardless of level of support (P < .01). Patients classified to a hyperinflammatory subphenotype at baseline (< 10%) showed worse 60-day survival (P < .0001) and 50% of them remained classified as hyperinflammatory at 5 days after enrollment.
Interpretation: Longitudinal study of the systemic host response in COVID-19 revealed substantial and predictive interindividual variability influenced by baseline levels of respiratory support.
Keywords: COVID-19; acute lung injury; acute respiratory failure; biomarkers; host response; longitudinal; subphenotypes.
Figures
Update of
-
Trajectories of host-response biomarkers and inflammatory subphenotypes in COVID-19 patients across the spectrum of respiratory support.medRxiv [Preprint]. 2022 Nov 29:2022.11.28.22282858. doi: 10.1101/2022.11.28.22282858. medRxiv. 2022. Update in: CHEST Crit Care. 2023 Dec;1(3):100018. doi: 10.1016/j.chstcc.2023.100018. PMID: 36482978 Free PMC article. Updated. Preprint.
Similar articles
-
Trajectories of host-response biomarkers and inflammatory subphenotypes in COVID-19 patients across the spectrum of respiratory support.medRxiv [Preprint]. 2022 Nov 29:2022.11.28.22282858. doi: 10.1101/2022.11.28.22282858. medRxiv. 2022. Update in: CHEST Crit Care. 2023 Dec;1(3):100018. doi: 10.1016/j.chstcc.2023.100018. PMID: 36482978 Free PMC article. Updated. Preprint.
-
Longitudinal respiratory subphenotypes in patients with COVID-19-related acute respiratory distress syndrome: results from three observational cohorts.Lancet Respir Med. 2021 Dec;9(12):1377-1386. doi: 10.1016/S2213-2600(21)00365-9. Epub 2021 Oct 13. Lancet Respir Med. 2021. PMID: 34653374 Free PMC article.
-
Subphenotypes in patients with acute respiratory distress syndrome treated with high-flow oxygen.Crit Care. 2023 Nov 1;27(1):419. doi: 10.1186/s13054-023-04687-0. Crit Care. 2023. PMID: 37915062 Free PMC article.
-
Safety and Efficacy of Imatinib for Hospitalized Adults with COVID-19: A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Oct 28;21(1):897. doi: 10.1186/s13063-020-04819-9. Trials. 2020. PMID: 33115543 Free PMC article.
-
Host-Response Subphenotypes Offer Prognostic Enrichment in Patients With or at Risk for Acute Respiratory Distress Syndrome.Crit Care Med. 2019 Dec;47(12):1724-1734. doi: 10.1097/CCM.0000000000004018. Crit Care Med. 2019. PMID: 31634231 Free PMC article.
Cited by
-
The utility of procalcitonin for identifying secondary infections in patients with influenza or COVID-19 receiving extracorporeal membrane oxygenation.Ther Adv Infect Dis. 2024 Jun 13;11:20499361241255873. doi: 10.1177/20499361241255873. eCollection 2024 Jan-Dec. Ther Adv Infect Dis. 2024. PMID: 38883923 Free PMC article.
-
Clinical and biologic profiles of patients with acute respiratory distress syndrome by prevalence of chronic obstructive pulmonary disease or emphysema; a cohort study.Respir Res. 2024 Nov 8;25(1):400. doi: 10.1186/s12931-024-03027-2. Respir Res. 2024. PMID: 39516808 Free PMC article.
-
Neutrophils and galectin-3 defend mice from lethal bacterial infection and humans from acute respiratory failure.Nat Commun. 2024 Jun 3;15(1):4724. doi: 10.1038/s41467-024-48796-y. Nat Commun. 2024. PMID: 38830855 Free PMC article.
-
Clinical Subtype Trajectories in Sepsis Patients Admitted to the ICU: A Secondary Analysis of an Observational Study.Crit Care Explor. 2024 Nov 14;6(11):e1176. doi: 10.1097/CCE.0000000000001176. eCollection 2024 Nov. Crit Care Explor. 2024. PMID: 39555471 Free PMC article.
-
Glucocorticoid use in acute respiratory failure from pulmonary causes and association with early changes in the systemic host immune response.Intensive Care Med Exp. 2024 Mar 5;12(1):24. doi: 10.1186/s40635-024-00605-y. Intensive Care Med Exp. 2024. PMID: 38441708 Free PMC article.
References
-
- World Health Organization. WHO coronavirus (COVID-19) dashboard. 2023. World Health Organization website. Accessed March 12, 2023. https://covid19.who.int/
-
- Centers for Disease Control and Prevention. COVID data tracker. 2023. Centers for Disease Control and Prevention website. Accessed March 12, 2023. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous