

Genetic and phenotypic analyses of PRRT2 positive and negative paroxysmal kinesigenic dyskinesia
- PMID: 38250317
- PMCID: PMC10798112
- DOI: 10.1177/17562864231224110
Genetic and phenotypic analyses of PRRT2 positive and negative paroxysmal kinesigenic dyskinesia
Abstract
Background: Paroxysmal kinesigenic dyskinesia (PKD) is a rare neurological disorder, characterized by attacks of involuntary movements triggered by sudden action. Variants in proline-rich transmembrane protein 2 (PRRT2) are the most common genetic cause of PKD.
Objective: The objective was to investigate the clinical and genetic characteristics of PKD and to establish genotype-phenotype correlations.
Methods: We enrolled 219 PKD patients, documented their clinical information and performed PRRT2 screening using Sanger sequencing. Whole exome sequencing was performed on 49 PKD probands without PRRT2 variants. Genotype-phenotype correlation analyses were conducted on the probands.
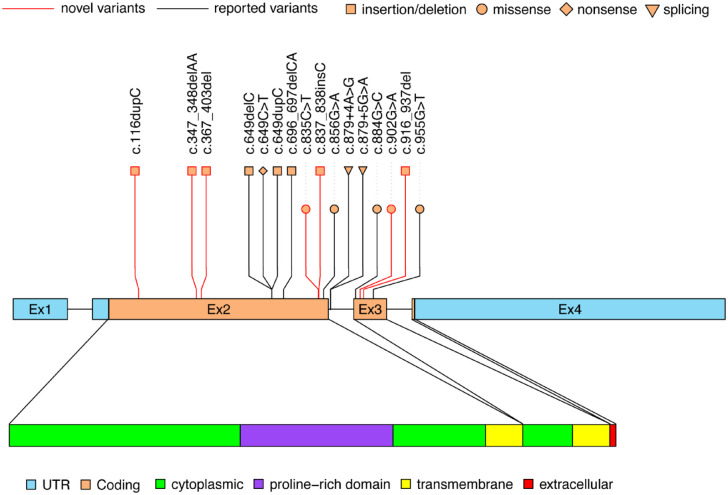
Results: Among 219 PKD patients (99 cases from 39 families and 120 sporadic cases), 16 PRRT2 variants were identified. Nine variants (c.879+4A>G, c.879+5G>A, c.856G>A, c.955G>T, c.884G>C, c.649C>T, c.649dupC, c.649delC and c.696_697delCA) were previously known, while seven were novel (c.367_403del, c.347_348delAA, c.835C>T, c.116dupC, c.837_838insC, c.916_937del and c.902G>A). The mean interval from onset to diagnosis was 7.94 years. Compared to patients without PRRT2 variants, patients with the variants were more likely to have a positive family history, an earlier age of onset and a higher prevalence of falls during pre-treatment attacks (27.14% versus 8.99%, respectively). Patients with truncated PRRT2 variants tend to have bilateral attacks. We identified two transmembrane protein 151A (TMEM151A) variants including a novel variant (c.368G>C) and a reported variant (c.203C>T) in two PRRT2-negative probands with PKD.
Conclusion: These findings provide insights on the clinical characteristics, diagnostic timeline and treatment response of PKD patients. PKD patients with truncated PRRT2 variants may tend to have more severe paroxysmal symptoms. This study expands the spectrum of PRRT2 and TMEM151A variants. Carbamazepine and oxcarbazepine are both used as a first-line treatment choice for PKD patients.
Keywords: PRRT2; carbamazepine; genotype–phenotype correlations; oxcarbazepine; paroxysmal kinesigenic dyskinesia.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures


References
-
- Bruno MK, Hallett M, Gwinn-Hardy K, et al.. Clinical evaluation of idiopathic paroxysmal kinesigenic dyskinesia: new diagnostic criteria. Neurology 2004; 63: 2280–2287. - PubMed
-
- Huang XJ, Wang SG, Guo XN, et al.. The phenotypic and genetic spectrum of paroxysmal kinesigenic dyskinesia in China. Mov Disord 2020; 35: 1428–1437. - PubMed
-
- Liu X, Ke H, Qian X, et al.. Clinical and genetic analyses of 150 patients with paroxysmal kinesigenic dyskinesia. J Neurol 2022; 269: 4717–4728. - PubMed
-
- Méneret A, Grabli D, Depienne C, et al.. PRRT2 mutations: a major cause of paroxysmal kinesigenic dyskinesia in the European population. Neurology 2012; 79: 170–174. - PubMed
LinkOut - more resources
Full Text Sources
