

Intra- and inter-fractional variations of tumors with fiducial markers measured using respiratory-correlated computed tomography images for respiratory gated lung stereotactic body radiation therapy
- PMID: 38252745
- PMCID: PMC11163493
- DOI: 10.1002/acm2.14280
Intra- and inter-fractional variations of tumors with fiducial markers measured using respiratory-correlated computed tomography images for respiratory gated lung stereotactic body radiation therapy
Abstract
Purpose: This study evaluated the intra- and inter-fractional variation of tumors with fiducial markers (FMs), relative to the tumor-FM distance, to establish how close an FM should be inserted for respiratory-gated stereotactic body radiation therapy (RG-SBRT).
Methods: Forty-five lung tumors treated with RG-SBRT were enrolled. End-expiratory computed tomography (CT) (CTplan) and four-dimensional-CT (4D-CT) scans were obtained for planning. End-expiratory CT (CTfr) scanning was performed before each fraction. The FMs were divided into two groups based on the median tumor-FM distance in the CTplan (Dp). For the intra-fractional variation, the correlations between the corresponding tumor and FM intra-fractional motions, defined as the centroid coordinates of those in each 0-90% phase, with the 50% phase of 4D-CT as the origin, were calculated in the left-right, anterior-posterior, and superior-inferior directions. Furthermore, the maximum difference in the tumor-FM distance in each phase of 4D-CT scan, based on those in the 50% phase of 4D-CT scan (Dmax), was obtained. Inter-fractional variation was defined as the maximum distance between the tumors in CTplan and CTfr, when the CT scans were fused based on each FM or vertebra.
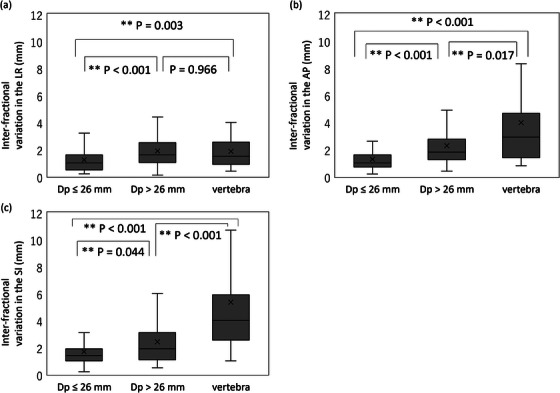
Results: The median Dp was 26.1 mm. While FM intra-fractional motions were significantly and strongly correlated with the tumor intra-fractional motions in only anterior-posterior and superior-inferior directions for the Dp > 26 mm group, they were significantly and strongly correlated in all directions for the Dp ≤ 26 mm group. In all directions, Dmax values of the Dp ≤ 26 mm group were lower than those of the Dp > 26 mm group. The inter-fractional variations based on the Dp ≤ 26 mm were smaller than those on the Dp > 26 mm and on the vertebra in all directions.
Conclusions: Regarding intra- and inter-fractional variation, FMs for Dp ≤ 26 mm can increase the accuracy for RG-SBRT.
Keywords: fiducial marker; lung tumor; stereotactic body radiation therapy.
© 2024 The Authors. Journal of Applied Clinical Medical Physics is published by Wiley Periodicals, Inc. on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
The authors have no conflicts of interest.
Figures




References
-
- Tateishi Y, Takeda A, Horita N, et al. Stereotactic body radiation therapy with a high maximum dose improves local control, cancer‐specific death, and overall survival in peripheral early‐stage non‐small cell lung cancer. Int J Radiat Oncol Biol Phys. 2021;111(1):143‐151. doi:10.1016/j.ijrobp.2021.04.014 - DOI - PubMed
-
- Oliver DE, Laborde JM, Singh DP, et al. Early‐stage primary lung neuroendocrine tumors treated with stereotactic body radiation therapy: a multi‐institution experience [published online ahead of print, 2023 Jan 26]. Int J Radiat Oncol Biol Phys. 2023;S0360‐3016(23):00071‐00078. doi:10.1016/j.ijrobp.2023.01.028 - DOI - PMC - PubMed
-
- Nagata Y, Hiraoka M, Shibata T, et al. Prospective trial of stereotactic body radiation therapy for both operable and inoperable T1N0M0 non‐small cell lung cancer: japan Clinical Oncology Group Study JCOG0403. Int J Radiat Oncol Biol Phys. 2015;93(5):989‐996. doi:10.1016/j.ijrobp.2015.07.2278 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
