

Efficacy and Safety of Respiratory Syncytial Virus (RSV) Prefusion F Protein Vaccine (RSVPreF3 OA) in Older Adults Over 2 RSV Seasons
- PMID: 38253338
- PMCID: PMC11175669
- DOI: 10.1093/cid/ciae010
Efficacy and Safety of Respiratory Syncytial Virus (RSV) Prefusion F Protein Vaccine (RSVPreF3 OA) in Older Adults Over 2 RSV Seasons
Abstract
Background: The adjuvanted RSV prefusion F protein-based vaccine (RSVPreF3 OA) was efficacious against RSV-related lower respiratory tract disease (RSV-LRTD) in ≥60-years-olds over 1 RSV season. We evaluated efficacy and safety of 1 RSVPreF3 OA dose and of 2 RSVPreF3 OA doses given 1 year apart against RSV-LRTD over 2 RSV seasons post-dose 1.
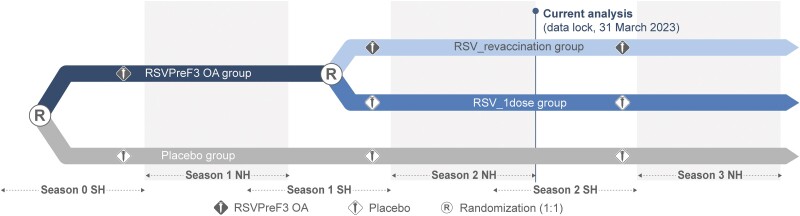
Methods: In this phase 3, blinded trial, ≥60-year-olds were randomized (1:1) to receive RSVPreF3 OA or placebo pre-season 1. RSVPreF3 OA recipients were re-randomized (1:1) to receive a second RSVPreF3 OA dose (RSV_revaccination group) or placebo (RSV_1dose group) pre-season 2; participants who received placebo pre-season 1 received placebo pre-season 2 (placebo group). Efficacy of both vaccine regimens against RSV-LRTD was evaluated over 2 seasons combined (confirmatory secondary objective, success criterion: lower limits of 2-sided CIs around efficacy estimates >20%).
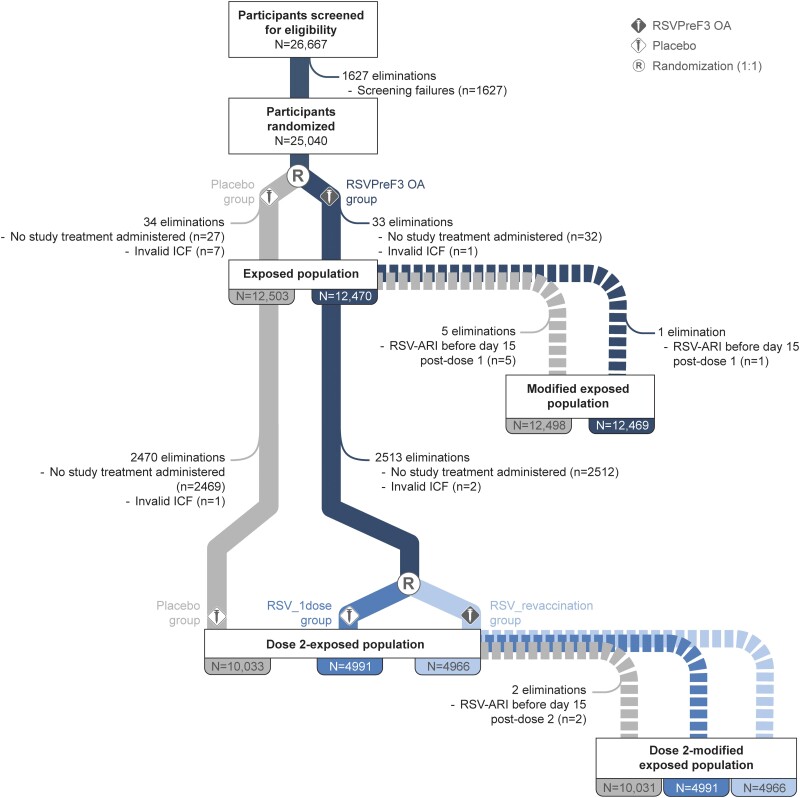
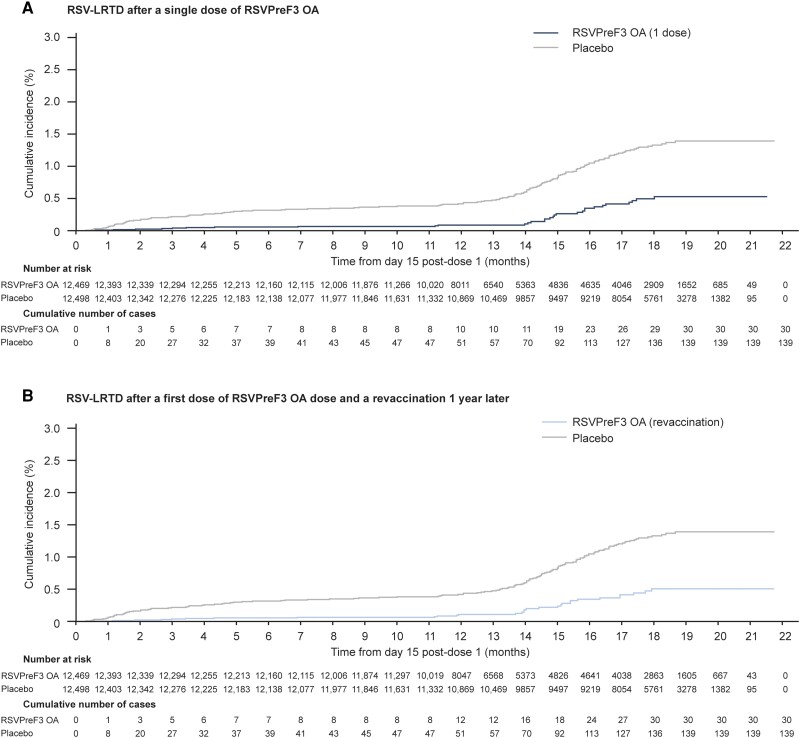
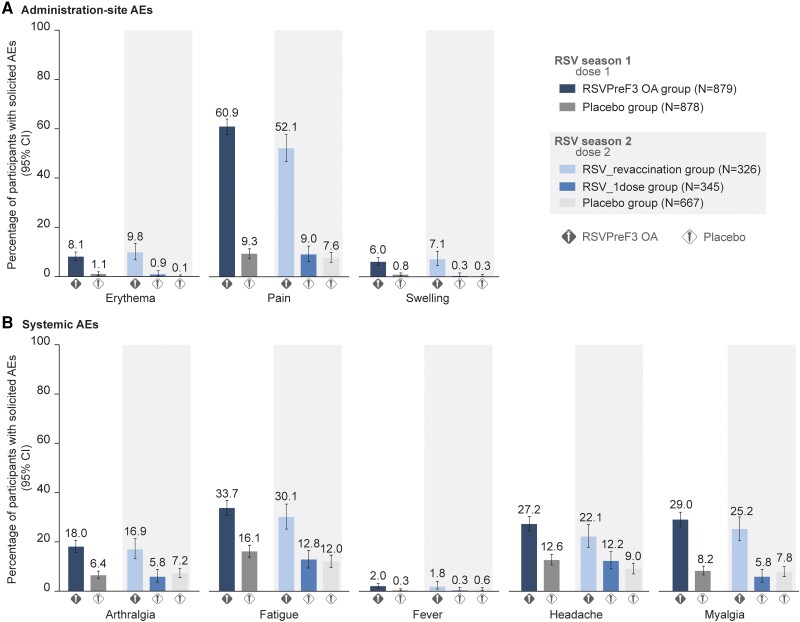
Results: The efficacy analysis comprised 24 967 participants (RSV_1dose: 6227; RSV_revaccination: 6242; placebo: 12 498). Median efficacy follow-up was 17.8 months. Efficacy over 2 seasons of 1 RSVPreF3 OA dose was 67.2% (97.5% CI: 48.2-80.0%) against RSV-LRTD and 78.8% (95% CI: 52.6-92.0%) against severe RSV-LRTD. Efficacy over 2 seasons of a first dose followed by revaccination was 67.1% (97.5% CI: 48.1-80.0%) against RSV-LRTD and 78.8% (95% CI: 52.5-92.0%) against severe RSV-LRTD. Reactogenicity/safety of the revaccination dose were similar to dose 1.
Conclusions: One RSVPreF3 OA dose was efficacious against RSV-LRTD over 2 RSV seasons in ≥60-year-olds. Revaccination 1 year post-dose 1 was well tolerated but did not seem to provide additional efficacy benefit in the overall study population.
Clinical trials registration: ClinicalTrials.gov: NCT04886596.
Keywords: RSV; older adults; respiratory syncytial virus prefusion F protein vaccine.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest . M. G. I. declares that research support from GSK was paid to his previous institution, Northwestern University; he received consulting fees from Adagio Therapeutics, ADMA Biologics, Adamis Pharmaceuticals, AlloVir, Atea, Cidara Therapeutics, Genentech/Roche, Janssen, Shionogi, Takeda, Talaris, and Eurofins Viracor; and payment for participating in data safety monitoring boards or advisory boards from Adamis Pharmaceuticals, AlloVir, National Institutes of Health, CSL Behring, Janssen, Merck, Seqirus, Takeda, and Talaris; all of these ended in December 2022; M. G. I. also receives author royalties from UpToDate, which is ongoing, and serves as Chair of the International Society for Influenza and other Respiratory Virus Diseases Antiviral Group and was Editor-in-Chief of Transplant Infectious Disease. A. P. declares funding from GSK for conducting the trial. A. P. also declares that his institution received grants from Chiesi, AstraZeneca, GSK, Sanofi, and Agenzia Italiana del Farmaco; that he received consulting fees from Chiesi, AstraZeneca, GSK, Novartis, Sanofi, Avillion, and ELPEN Pharmaceuticals; payment for participation in advisory boards from Chiesi, AstraZeneca, GSK, Novartis, Sanofi, IQVIA, Avillion, and ELPEN Pharmaceuticals; and honoraria from Chiesi, AstraZeneca, GSK, Menarini, Novartis, Zambon, Mundipharma, Sanofi, Edmond Pharmaceuticals, IQVIA, Avillion, and ELPEN Pharmaceuticals. R. G. F. declares having received payment from GSK for lectures and support for travel related to these activities. J. M. L. reports grants from GSK paid to her institution for the conduct of the trial and from GSK, Pfizer, Merck, Moderna, Sanofi, Inventprise, and VBI Vaccines for other trials; J. M. L. also reports being a board member of Seqirus and participating on a data safety monitoring board or advisory board for Vaxcyte; she is an expert panelist for Canada's Drug and Health Technology Agency for the review of nirsevimab. I. L.-R. declares that her institution received funding from GSK for conducting this trial; from Icosavax, Virometix, Janssen Vaccines, Curevac, Moderna, Osivax, MSD, ICON Genetics, and OSE Immunotherapeutics for other vaccine trials; from Janssen Vaccines and MSD for consulting services; and from Janssen Vaccines for participation on a data safety monitoring board or advisory board. F. M.-T. declares that his institution received payment from GSK for conducting this trial and from Ablynx, Abbott, Seqirus, Sanofi, MSD, Merck, Pfizer, Roche, Regeneron, Janssen, Medimmune, Novavax, Novartis, and GSK for other vaccine trials; F. M.-T. also reports receiving honoraria for lectures from Sanofi, MSD, Moderna, GSK, Biofabri, AstraZeneca, Novavax, Janssen, and Pfizer; payment of travel expenses and meeting fees from Pfizer, MSD, GSK, and Sanofi; and participation on data safety monitoring boards or advisory boards for Pfizer and Biofabri; F. M.-T. is also a member of the World Health Organization’s (WHO's) European Technical Advisory Group of Experts, coordinator of the Spanish Pediatric Clinical Trials Network, and coordinator of the WHO Collaborating Center for Vaccine Safety of Santiago de Compostela. T. F. S. reports honoraria and/or participation on data safety monitoring boards or advisory boards from Alexion, AstraZeneca, Bavarian Nordic, Biogen, Biontech, GSK, Janssen-Cilag, Merck-Serono, Moderna, MSD, Novavax, Pfizer, Roche, Sanofi-Aventis, Seqirus, Synlab, Takeda, and va-Q-tec. R. N. v. Z.-S. reports that his institution received support from Boehringer Ingelheim for the Interstitial Lung Diseases (ILD) registry and that he received consulting fees from GSK and honoraria for lectures from Glenmark, Boehringer Ingelheim, Cipla, and Novartis; R. N. v. Z.-S. also participated on data safety monitoring boards or advisory boards for OnQ SA; he is president of the South African Thoracic Society and co-chair of the International Health Committee of the American Thoracic Society. C. V., N. D., O. G., L. F., M.-P. D., L. K., V. H., A. O., M. V. d. W., and D. D. are employed by GSK and have stock options or shares from GSK. N. D. is co-applicant on a pending patent for vaccination against RSV and has stock options from Haleon. L. F., M.-P. D., A. O., and M. V. d. W. are co-applicants on a pending patent filed by GSK. The other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

References
-
- Li Y, Reeves RM, Wang X, et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: a systematic analysis. Lancet Glob Health 2019; 7:e1031–45. - PubMed
-
- Nam HH, Ison MG. Respiratory syncytial virus infection in adults. BMJ 2019; 366:l5021. - PubMed
-
- Branche AR, Saiman L, Walsh EE, et al. Incidence of respiratory syncytial virus infection among hospitalized adults, 2017–2020. Clin Infect Dis 2022; 74:1004–11. - PubMed
