A Contemporary Approach to the Diagnosis and Management of Adrenal Insufficiency
- PMID: 38253474
- PMCID: PMC10901672
- DOI: 10.3803/EnM.2024.1894
A Contemporary Approach to the Diagnosis and Management of Adrenal Insufficiency
Abstract
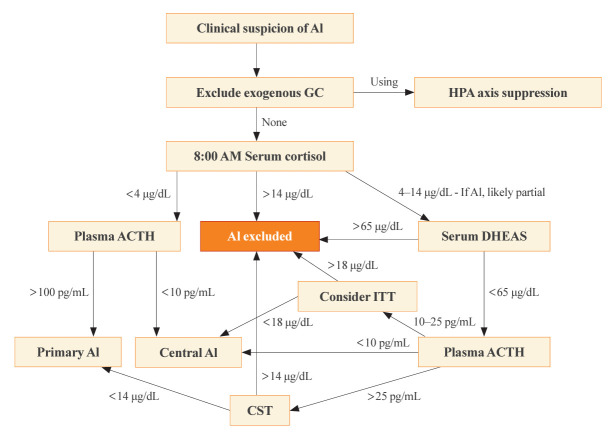
Adrenal insufficiency (AI) can be classified into three distinct categories based on its underlying causes: primary adrenal disorders, secondary deficiencies in adrenocorticotropin, or hypothalamic suppression from external factors, most commonly glucocorticoid medications used for anti-inflammatory therapy. The hallmark clinical features of AI include fatigue, appetite loss, unintentional weight loss, low blood pressure, and hyponatremia. Individuals with primary AI additionally manifest skin hyperpigmentation, hyperkalemia, and salt craving. The diagnosis of AI is frequently delayed due to the non-specific symptoms and signs early in the disease course, which poses a significant challenge to its early detection prior to an adrenal crisis. Despite the widespread availability of lifesaving glucocorticoid medications for decades, notable challenges persist, particularly in the domains of timely diagnosis while simultaneously avoiding misdiagnosis, patient education for averting adrenal crises, and the determination of optimal replacement therapies. This article reviews recent advancements in the contemporary diagnostic strategy and approaches to optimal treatment for AI.
Keywords: Adrenal cortex; Adrenal insufficiency; Glucocorticoids; Mineralocorticoids.
Conflict of interest statement
Richard J. Auchus reports consulting fees and contracted research support from Diurnal, Ltd. and Neurocrine Biosciences. Suranut Charoensri has nothing to declare.
Figures
Similar articles
-
Primary adrenal insufficiency in children: Diagnosis and management.Best Pract Res Clin Endocrinol Metab. 2018 Aug;32(4):397-424. doi: 10.1016/j.beem.2018.05.010. Epub 2018 Jun 6. Best Pract Res Clin Endocrinol Metab. 2018. PMID: 30086866 Review.
-
Adrenal insufficiency - causes and laboratory diagnosis.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2025 Jun;169(2):73-81. doi: 10.5507/bp.2024.033. Epub 2024 Oct 7. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2025. PMID: 39380209 Review.
-
Treatment and Follow-up of Non-stress Adrenal Insufficiency.J Clin Res Pediatr Endocrinol. 2025 Jan 10;17(Suppl 1):93-101. doi: 10.4274/jcrpe.galenos.2024.2024-6-23-S. Epub 2024 Dec 23. J Clin Res Pediatr Endocrinol. 2025. PMID: 39713906 Free PMC article. Review.
-
[Adrenal insufficiency of the adult].Rev Med Interne. 2016 Dec;37(12):820-826. doi: 10.1016/j.revmed.2016.02.007. Epub 2016 Mar 22. Rev Med Interne. 2016. PMID: 27016277 French.
-
Factors impacting on the action of glucocorticoids in patients receiving glucocorticoid therapy.Clin Endocrinol (Oxf). 2019 Jan;90(1):3-14. doi: 10.1111/cen.13837. Epub 2018 Sep 24. Clin Endocrinol (Oxf). 2019. PMID: 30120786 Review.
Cited by
-
A deep learning algorithm for automated adrenal gland segmentation on non-contrast CT images.BMC Med Imaging. 2025 May 1;25(1):142. doi: 10.1186/s12880-025-01682-5. BMC Med Imaging. 2025. PMID: 40312690 Free PMC article.
-
Adrenal Insufficiency in Patients with Beta Thalassemia: A Meta-Analysis.Medicina (Kaunas). 2024 Sep 25;60(10):1571. doi: 10.3390/medicina60101571. Medicina (Kaunas). 2024. PMID: 39459358 Free PMC article.
References
-
- Hahner S, Ross RJ, Arlt W, Bancos I, Burger-Stritt S, Torpy DJ, et al. Adrenal insufficiency. Nat Rev Dis Primers. 2021;7:19. - PubMed
-
- Husebye ES, Pearce SH, Krone NP, Kampe O. Adrenal insufficiency. Lancet. 2021;397:613–29. - PubMed
-
- Barthel A, Benker G, Berens K, Diederich S, Manfras B, Gruber M, et al. An update on Addison’s disease. Exp Clin Endocrinol Diabetes. 2019;127:165–75. - PubMed
-
- Fleseriu M, Hashim IA, Karavitaki N, Melmed S, Murad MH, Salvatori R, et al. Hormonal replacement in hypopituitarism in adults: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2016;101:3888–921. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical