

Hypofractionated Radiotherapy in Gynecologic Malignancies-A Peek into the Upcoming Evidence
- PMID: 38254851
- PMCID: PMC10814353
- DOI: 10.3390/cancers16020362
Hypofractionated Radiotherapy in Gynecologic Malignancies-A Peek into the Upcoming Evidence
Abstract
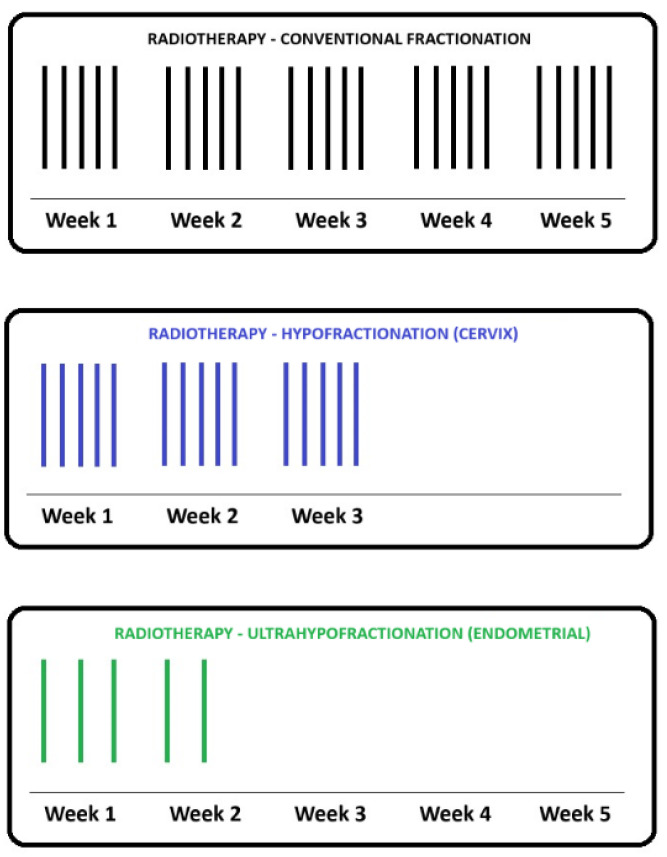
Radiotherapy (RT) has a fundamental role in the treatment of gynecologic malignancies, including cervical and uterine cancers. Hypofractionated RT has gained popularity in many cancer sites, boosted by technological advances in treatment delivery and image verification. Hypofractionated RT uptake was intensified during the COVID-19 pandemic and has the potential to improve universal access to radiotherapy worldwide, especially in low-resource settings. This review summarizes the rationale, the current challenges and investigation efforts, together with the recent developments associated with hypofractionated RT in gynecologic malignancies. A comprehensive search was undertaken using multiple databases and ongoing trial registries. In the definitive radiotherapy setting for cervical cancers, there are several ongoing clinical trials from Canada, Mexico, Iran, the Philippines and Thailand investigating the role of a moderate hypofractionated external beam RT regimen in the low-risk locally advanced population. Likewise, there are ongoing ultra and moderate hypofractionated RT trials in the uterine cancer setting. One Canadian prospective trial of stereotactic hypofractionated adjuvant RT for uterine cancer patients suggested a good tolerance to this treatment strategy in the acute setting, with a follow-up trial currently randomizing patients between conventional fractionation and the hypofractionated dose regimen delivered in the former trial. Although not yet ready for prime-time use, hypofractionated RT could be a potential solution to several challenges that limit access to and the utilization of radiotherapy for gynecologic cancer patients worldwide.
Keywords: cervical cancer; gynecologic malignancies; hypofractionated radiotherapy; universal access to radiotherapy; uterine cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- McCall N.S., Eng T.Y., Shelton J.W., Hanasoge S., Patel P.R., Patel A.B., Jr., McCook-Veal A.A., Switchenko J.M., Cole T.E., Khanna N., et al. Incidence and Predictors of Toxicity in the Management of Vulvar Squamous Cell Carcinoma Treated with Radiation Therapy. Gynecol. Oncol. Rep. 2022;44:101086. doi: 10.1016/j.gore.2022.101086. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
