

Stratification of COVID-19 Patients with Moderate-to-Severe Hypoxemic Respiratory Failure for Response to High-Flow Nasal Cannula: A Retrospective Observational Study
- PMID: 38256332
- PMCID: PMC10819134
- DOI: 10.3390/medicina60010071
Stratification of COVID-19 Patients with Moderate-to-Severe Hypoxemic Respiratory Failure for Response to High-Flow Nasal Cannula: A Retrospective Observational Study
Abstract
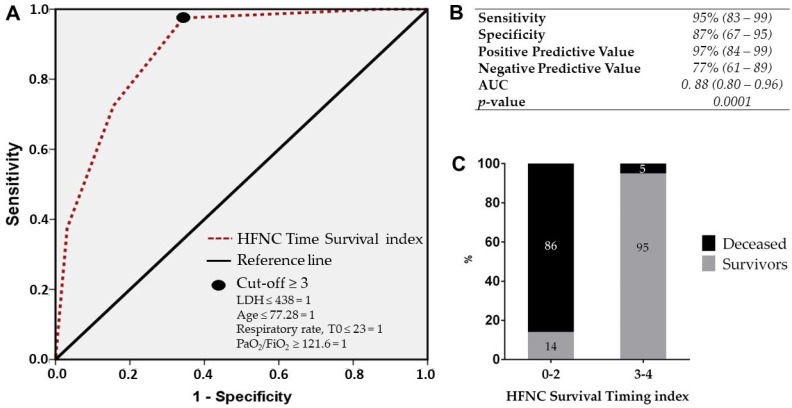
Background and Objectives: In patients with COVID-19, high-flow nasal cannula (HFNC) and continuous positive airway pressure (CPAP) are widely applied as initial treatments for moderate-to-severe acute hypoxemic respiratory failure. The aim of the study was to assess which respiratory supports improve 28-day mortality and to identify a predictive index of treatment response. Materials and Methods: This is a single-center retrospective observational study including 159 consecutive adult patients with COVID-19 and moderate-to-severe hypoxemic acute respiratory failure. Results: A total of 159 patients (82 in the CPAP group and 77 in the HFNC group) were included in the study. Mortality within 28 days was significantly lower with HFNC compared to CPAP (16.8% vs. 50%), while ICU admission and tracheal intubation within 28 days were significantly higher with CPAP compared to HFNC treatment (32% vs. 13%). We identified an index for survival in HFNC by including three variables easily available at admission (LDH, age, and respiratory rate) and the PaO2/FiO2 ratio at 48 h. The index showed high discrimination for survival with an AUC of 0.88, a negative predictive value of 86%, and a positive predictive value of 95%. Conclusions: Treatment with HFNC appears to be associated with greater survival and fewer ICU admission than CPAP. LDH, respiratory rate, age, and PaO2/FiO2 at 48 h were independently associated with survival and an index based on these variables allows for the prediction of treatment success and the assessment of patient allocation to the appropriate intensity of care after 48 h. Further research is warranted to determine effects on other outcomes and to assess the performance of the index in larger cohorts.
Keywords: COVID-19; CPAP; HFNC; NIRS; NIV; mortality.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures



Similar articles
-
Effect of the Early Combination of Continuous Positive Airway Pressure and High-Flow Nasal Cannula on Mortality and Intubation Rates in Patients With COVID-19 and Acute Respiratory Distress Syndrome. The DUOCOVID Study.Arch Bronconeumol. 2023 May;59(5):288-294. doi: 10.1016/j.arbres.2023.01.009. Epub 2023 Feb 2. Arch Bronconeumol. 2023. PMID: 36797139 Free PMC article.
-
Comparison between high-flow nasal cannula and noninvasive ventilation in COVID-19 patients: a systematic review and meta-analysis.Ther Adv Respir Dis. 2022 Jan-Dec;16:17534666221113663. doi: 10.1177/17534666221113663. Ther Adv Respir Dis. 2022. PMID: 35861299 Free PMC article.
-
Continuous positive airway pressure versus high-flow nasal cannula oxygen therapy for acute hypoxemic respiratory failure: A randomized controlled trial.Respirology. 2024 Jan;29(1):36-45. doi: 10.1111/resp.14588. Epub 2023 Aug 30. Respirology. 2024. PMID: 37648252 Clinical Trial.
-
ROX index and SpO2/FiO2 ratio for predicting high-flow nasal cannula failure in hypoxemic COVID-19 patients: A multicenter retrospective study.PLoS One. 2022 May 12;17(5):e0268431. doi: 10.1371/journal.pone.0268431. eCollection 2022. PLoS One. 2022. PMID: 35551328 Free PMC article.
-
Comparison between high-flow nasal cannula and conventional oxygen therapy in COVID-19 patients: a systematic review and meta-analysis.Ther Adv Respir Dis. 2024 Jan-Dec;18:17534666231225323. doi: 10.1177/17534666231225323. Ther Adv Respir Dis. 2024. PMID: 38230522 Free PMC article.
Cited by
-
Editorial for the Special Issue "Emergency Medicine and Emergency Room Medical Issues II".Medicina (Kaunas). 2024 Mar 25;60(4):530. doi: 10.3390/medicina60040530. Medicina (Kaunas). 2024. PMID: 38674176 Free PMC article.
-
Comparative Effectiveness of High-Flow Nasal Cannula and Noninvasive Ventilation in Acute Hypoxemic Respiratory Failure: A Scoping Review.Cureus. 2025 May 8;17(5):e83752. doi: 10.7759/cureus.83752. eCollection 2025 May. Cureus. 2025. PMID: 40486342 Free PMC article. Review.
References
-
- Bellani G., Laffey J.G., Pham T., Fan E., Brochard L., Esteban A., Gattinoni L., van Haren F., Larsson A., McAuley D.F., et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA. 2016;315:788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Koch V., Gruenewald L.D., Albrecht M.H., Eichler K., Gruber-Rouh T., Yel I., Alizadeh L.S., Mahmoudi S., Scholtz J.E., Martin S.S., et al. Lung Opacity and Coronary Artery Calcium Score: A Combined Tool for Risk Stratification and Outcome Prediction in COVID-19 Patients. Acad. Radiol. 2022;29:861–870. doi: 10.1016/j.acra.2022.02.019. - DOI - PMC - PubMed
-
- Knight S.R., Ho A., Pius R., Buchan I., Carson G., Drake T.M., Dunning J., Fairfield C.J., Gamble C., Green C.A., et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ. 2020;370:m3339. doi: 10.1136/bmj.m3339. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
