

Redefining the Axillary Aesthetic: Surgical Management of Axillary Tissue Hypertrophy
- PMID: 38256387
- PMCID: PMC10821127
- DOI: 10.3390/medicina60010126
Redefining the Axillary Aesthetic: Surgical Management of Axillary Tissue Hypertrophy
Abstract
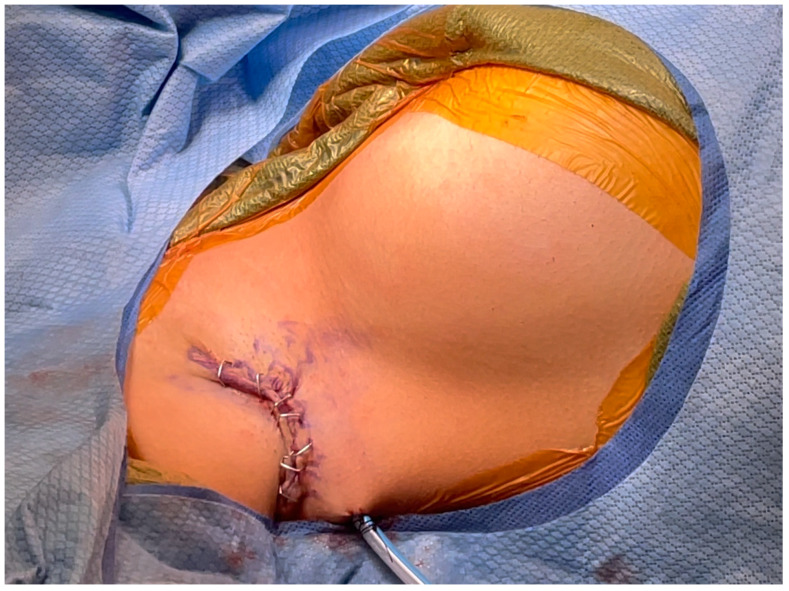
Background and Objectives: Axillary tissue hypertrophy consists of ectopic breast tissue and occurs in up to six percent of women. Women complain of pain, interference with activity, and dissatisfaction with appearance. While it is recommended that accessory breast tissue be removed via surgical excision, there is lack of consensus on the best technique for the surgical management of axillary tissue hypertrophy. In this study, the senior authors (BC and NT) review outcomes and complications as they pertain to the surgical treatment of axillary tissue hypertrophy and axillary contouring. Materials and Methods: A retrospective review of all patients (n = 35), from two separate institutions, who presented with axillary tissue hypertrophy between December 2019 and August 2021 was conducted. All patients underwent a technique that included direct crescentic dermato-lipectomy and glandular excision with axillary crease obliteration. Tissue was sent for histological analysis after removal. During a six-month follow-up period, all patient outcomes were recorded. Results: The authors treated 35 women with axillary tissue hypertrophy. All patients complained of aesthetic deformity with significant discomfort leading to the desire for surgery. Histologically, all specimens contained benign breast and adipose tissue. Hypertrophic scarring, seroma, and axillary cording were noted complications. Conclusions: Detailed is the surgical management and optimal technique that can be used to treat both adipose and fibroglandular axillary tissue hypertrophy while simultaneously providing a favorable axillary aesthetic.
Keywords: aesthetic surgery; axillary tissue; breast surgery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
-
- Schoenwolf G.C., Bleyl S.B., Brauer P.R., Francis-West P.H. Development of the skin and its derivatives. In: Larsen W.J., editor. Human Embryology. 4th ed. Churchill Livingstone; Philadelphia, PA, USA: 2009. pp. 193–216.
-
- Sahu S.K., Husain M., Sachan P.K. Bilateral accessory breast. Internet J. Surg. 2008
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
