

Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting
- PMID: 38257141
- PMCID: PMC10820062
- DOI: 10.3390/nu16020246
Metabolic and Nutritional Issues after Lower Digestive Tract Surgery: The Important Role of the Dietitian in a Multidisciplinary Setting
Abstract
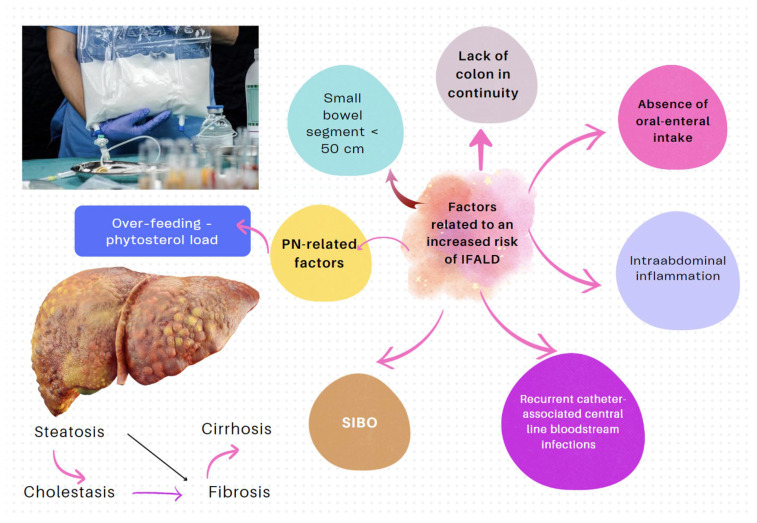
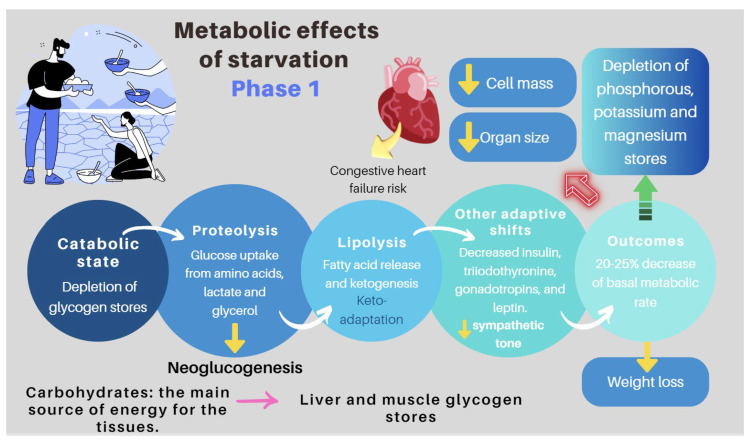
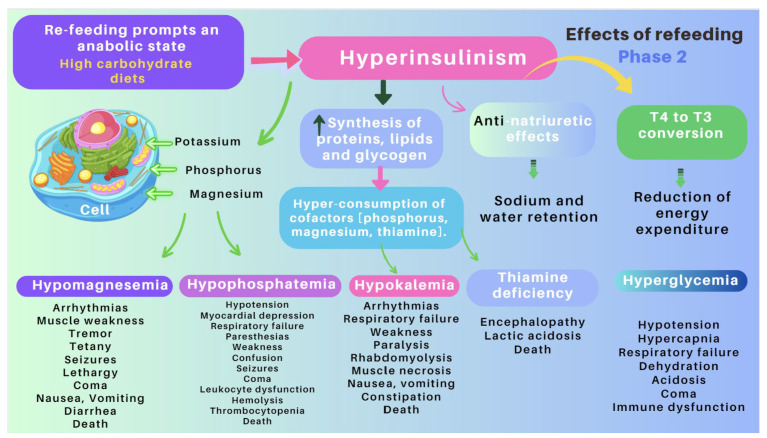
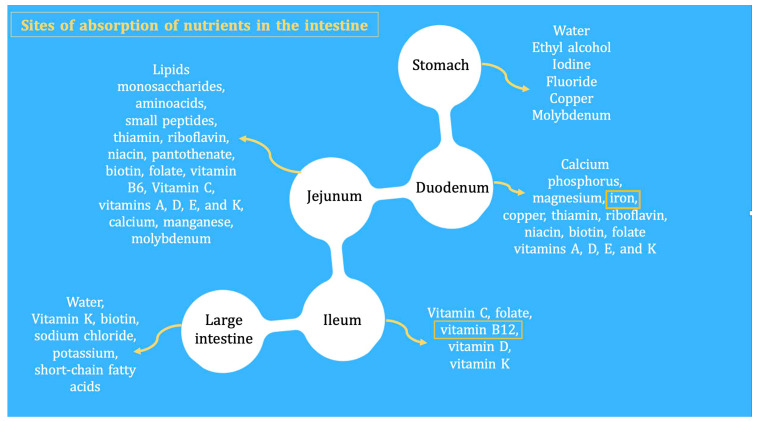
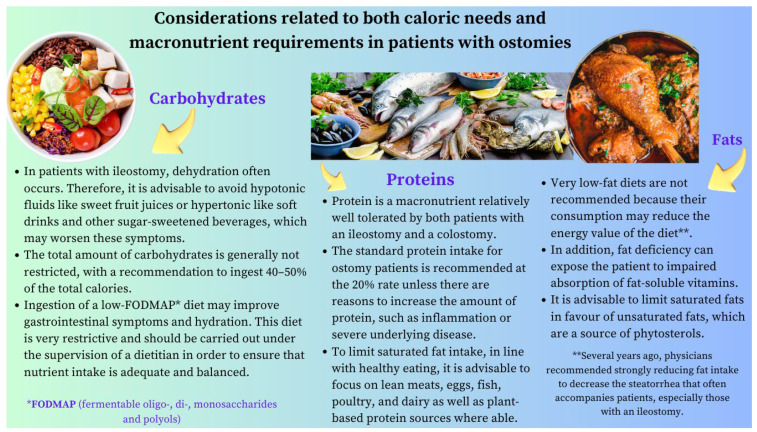
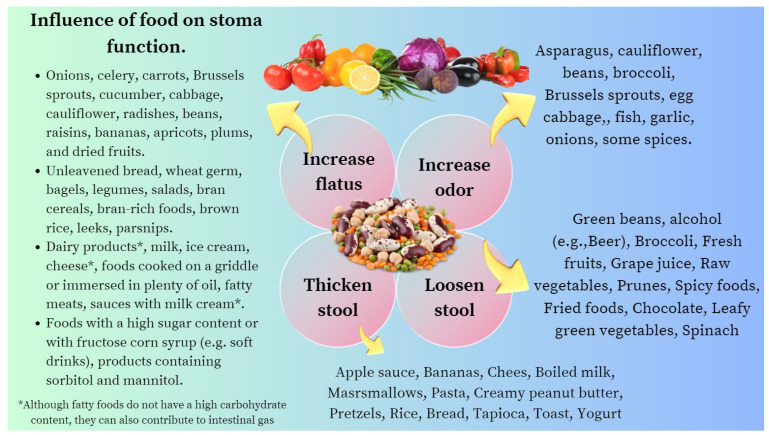
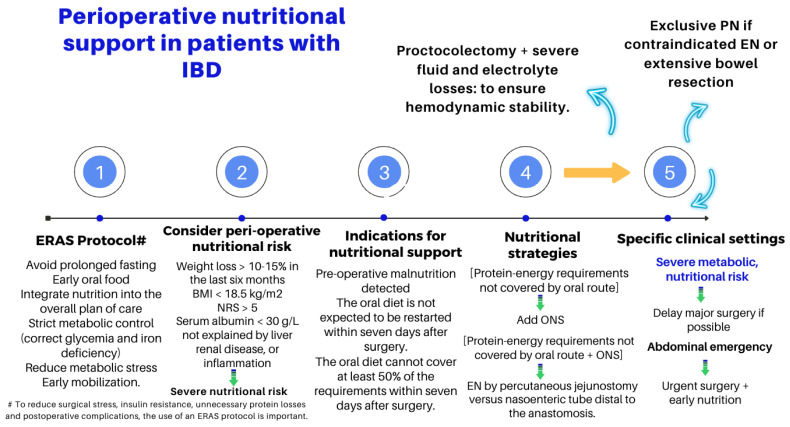
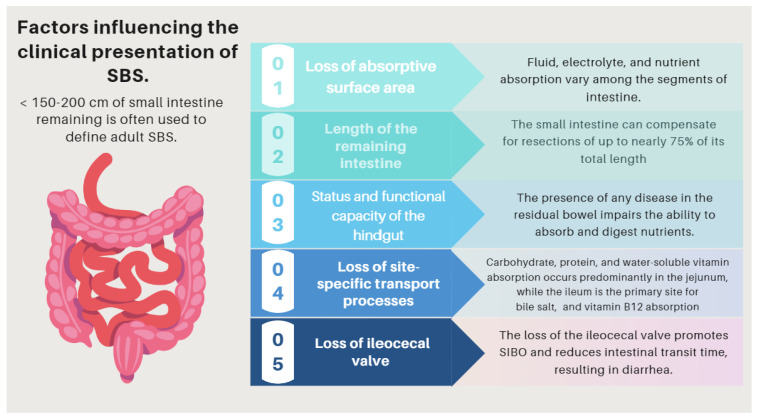
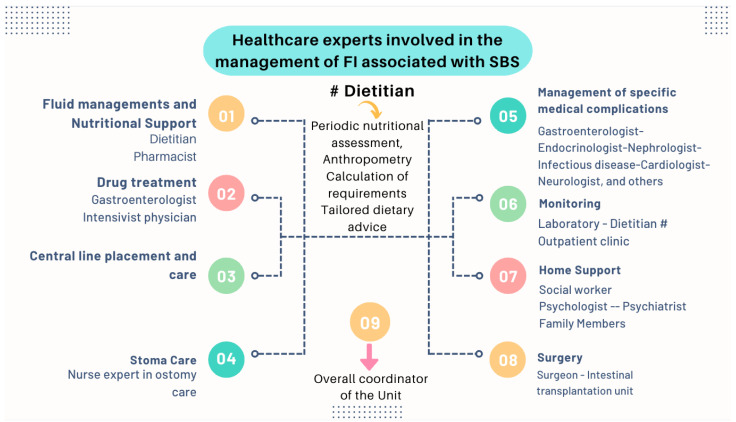
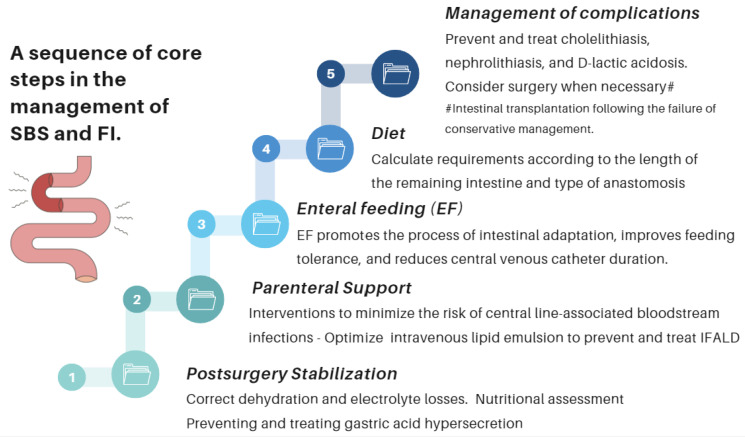
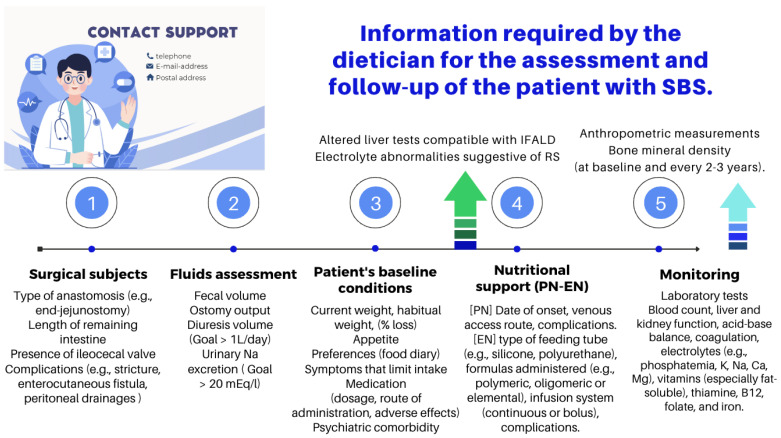
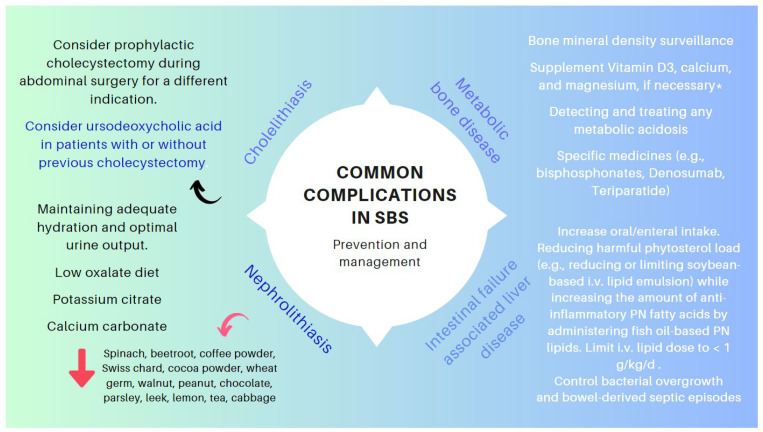
Many patients undergo small bowel and colon surgery for reasons related to malignancy, inflammatory bowel disease (IBD), mesenteric ischemia, and other benign conditions, including post-operative adhesions, hernias, trauma, volvulus, or diverticula. Some patients arrive in the operating theatre severely malnourished due to an underlying disease, while others develop complications (e.g., anastomotic leaks, abscesses, or strictures) that induce a systemic inflammatory response that can increase their energy and protein requirements. Finally, anatomical and functional changes resulting from surgery can affect either nutritional status due to malabsorption or nutritional support (NS) pathways. The dietitian providing NS to these patients needs to understand the pathophysiology underlying these sequelae and collaborate with other professionals, including surgeons, internists, nurses, and pharmacists. The aim of this review is to provide an overview of the nutritional and metabolic consequences of different types of lower gastrointestinal surgery and the role of the dietitian in providing comprehensive patient care. This article reviews the effects of small bowel resection on macronutrient and micronutrient absorption, the effects of colectomies (e.g., ileocolectomy, low anterior resection, abdominoperineal resection, and proctocolectomy) that require special dietary considerations, nutritional considerations specific to ostomized patients, and clinical practice guidelines for caregivers of patients who have undergone a surgery for local and systemic complications of IBD. Finally, we highlight the valuable contribution of the dietitian in the challenging management of short bowel syndrome and intestinal failure.
Keywords: D-lactic acidosis; IBD; IF-associated liver disease; abdominoperineal resection; colectomy; dietitian; enteral nutrition; health costs; home parenteral nutrition; intestinal failure (IF); intestinal transplantation; low anterior resection; malnutrition; metabolism; micronutrients; nutrition assessment; nutritional deficiencies; proctocolectomy; refeeding syndrome; short bowel syndrome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
AGA Clinical Practice Update on Diet and Nutritional Therapies in Patients With Inflammatory Bowel Disease: Expert Review.Gastroenterology. 2024 Mar;166(3):521-532. doi: 10.1053/j.gastro.2023.11.303. Epub 2024 Jan 23. Gastroenterology. 2024. PMID: 38276922
-
Feeding the critically ill obese patient: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):95-109. doi: 10.11124/jbisrir-2015-2458. JBI Database System Rev Implement Rep. 2015. PMID: 26571286
-
Nutritional deficiencies in inflammatory bowel disease: therapeutic approaches.Clin Nutr. 2013 Dec;32(6):904-10. doi: 10.1016/j.clnu.2013.03.020. Epub 2013 Apr 6. Clin Nutr. 2013. PMID: 23602613 Review.
-
Perioperative Dietary Therapy in Inflammatory Bowel Disease.J Crohns Colitis. 2020 May 21;14(4):431-444. doi: 10.1093/ecco-jcc/jjz160. J Crohns Colitis. 2020. PMID: 31550347
-
Small and Large Intestine (II): Inflammatory Bowel Disease, Short Bowel Syndrome, and Malignant Tumors of the Digestive Tract.Nutrients. 2021 Jul 6;13(7):2325. doi: 10.3390/nu13072325. Nutrients. 2021. PMID: 34371835 Free PMC article. Review.
Cited by
-
Prevalence and trends of cancer-related daily life limitations among gastrointestinal cancer survivors.J Cancer Surviv. 2025 May 24. doi: 10.1007/s11764-025-01833-1. Online ahead of print. J Cancer Surviv. 2025. PMID: 40411677
-
Enhancements in Parkinson's Disease Management: Leveraging Levodopa Optimization and Surgical Breakthroughs.Curr Drug Targets. 2025;26(1):17-32. doi: 10.2174/0113894501319817240919103802. Curr Drug Targets. 2025. PMID: 39350551 Review.
-
PERIOPERATIVE NUTRITIONAL SUPPORT IN GASTROINTESTINAL SURGERY - WHY IS IT ESSENTIAL?Arq Gastroenterol. 2025 Jun 16;62:e24094. doi: 10.1590/S0004-2803.24612024-94. eCollection 2025. Arq Gastroenterol. 2025. PMID: 40531682 Free PMC article. Review.
References
-
- Canzan F., Caliaro A., Cavada M.L., Mezzalira E., Paiella S., Ambrosi E. The effect of early oral postoperative feeding on the recovery of intestinal motility after gastrointestinal surgery: Protocol for a systematic review and meta-analysis. PLoS ONE. 2022;17:e0273085. doi: 10.1371/journal.pone.0273085. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
