

Clofazimine as a substitute for rifampicin improves efficacy of Mycobacterium avium pulmonary disease treatment in the hollow-fiber model
- PMID: 38259101
- PMCID: PMC10916390
- DOI: 10.1128/aac.01157-23
Clofazimine as a substitute for rifampicin improves efficacy of Mycobacterium avium pulmonary disease treatment in the hollow-fiber model
Abstract
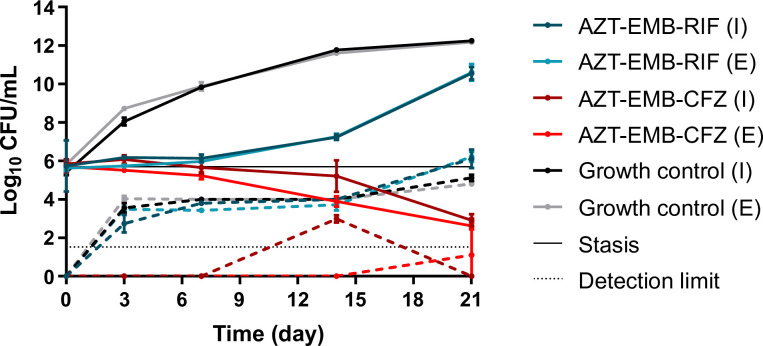
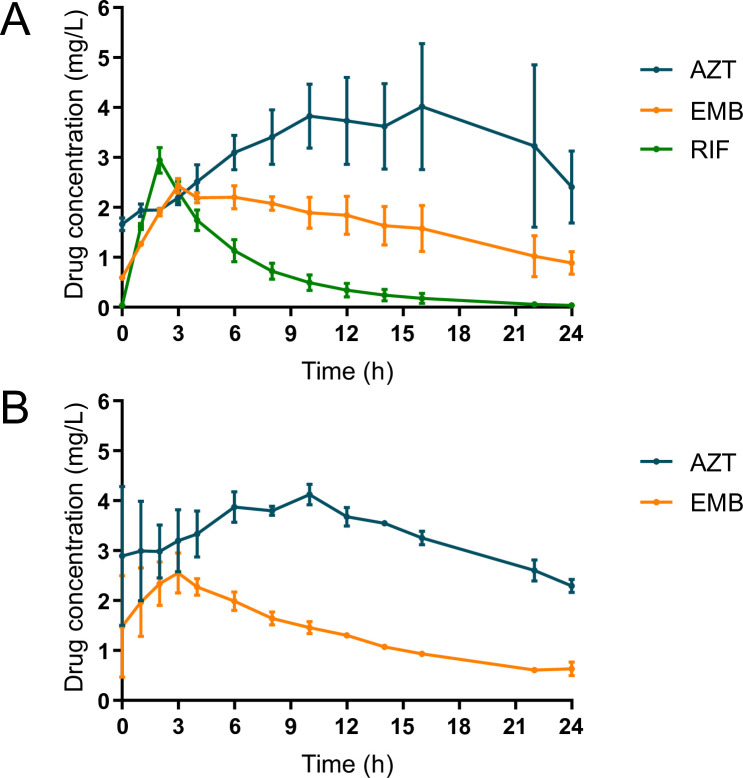
Mycobacterium avium complex pulmonary disease is treated with an azithromycin, ethambutol, and rifampicin regimen, with limited efficacy. The role of rifampicin is controversial due to inactivity, adverse effects, and drug interactions. Here, we evaluated the efficacy of clofazimine as a substitute for rifampicin in an intracellular hollow-fiber infection model. THP-1 cells, which are monocytes isolated from peripheral blood from an acute monocytic leukemia patient, were infected with M. avium ATCC 700898 and exposed to a regimen of azithromycin and ethambutol with either rifampicin or clofazimine. Intrapulmonary pharmacokinetic profiles of azithromycin, ethambutol, and rifampicin were simulated. For clofazimine, a steady-state average concentration was targeted. Drug concentrations and bacterial densities were monitored over 21 days. Exposures to azithromycin and ethambutol were 20%-40% lower than targeted but within clinically observed ranges. Clofazimine exposures were 1.7 times higher than targeted. Until day 7, both regimens were able to maintain stasis. Thereafter, regrowth was observed for the rifampicin-containing regimen, while the clofazimine-containing regimen yielded a 2 Log10 colony forming unit (CFU) per mL decrease in bacterial load. The clofazimine regimen also successfully suppressed the emergence of macrolide tolerance. In summary, substitution of rifampicin with clofazimine in the hollow-fiber model improved the antimycobacterial activity of the regimen. Clofazimine-containing regimens merit investigation in clinical trials.
Keywords: PK/PD; clofazimine; hollow-fiber infection model; nontuberculous mycobacteria; pharmacodynamics; pharmacokinetics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Daley CL, Iaccarino JM, Lange C, Cambau E, Wallace RJ Jr, Andrejak C, Böttger EC, Brozek J, Griffith DE, Guglielmetti L, Huitt GA, Knight SL, Leitman P, Marras TK, Olivier KN, Santin M, Stout JE, Tortoli E, van Ingen J, Wagner D, Winthrop KL. 2020. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J 56:2000535. doi:10.1183/13993003.00535-2020 - DOI - PMC - PubMed
-
- Fröberg G, Maurer FP, Chryssanthou E, Fernström L, Benmansour H, Boarbi S, Mengshoel AT, Keller PM, Viveiros M, Machado D, et al. . 2023. Towards clinical breakpoints for non-tuberculous mycobacteria – determination of epidemiological cut off values for the Mycobacterium avium complex and Mycobacterium abscessus using broth microdilution. Clin Microbiol Infect 29:758–764. doi:10.1016/j.cmi.2023.02.007 - DOI - PubMed
-
- van Ingen J, Aliberti S, Andrejak C, Chalmers JD, Codecasa LR, Daley CL, Hasegawa N, Griffith DE, Hoefsloot W, Huitt G, Jarand J, Jhun BW, Loebinger MR, Marras TK, Morimoto K, Polverino E, Ringshausen FC, Santin M, Thomson R, Wagner D, Wallace RJ, Winthrop KL, Yim J-J. 2021. Management of drug toxicity in Mycobacterium avium complex pulmonary disease: an expert panel survey. Clin Infect Dis 73:e256–e259. doi:10.1093/cid/ciaa1361 - DOI - PMC - PubMed
-
- van Ingen J, Egelund EF, Levin A, Totten SE, Boeree MJ, Mouton JW, Aarnoutse RE, Heifets LB, Peloquin CA, Daley CL. 2012. The pharmacokinetics and pharmacodynamics of pulmonary Mycobacterium avium complex disease treatment. Am J Respir Crit Care Med 186:559–565. doi:10.1164/rccm.201204-0682OC - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
