

Functional Outcomes After Localized Prostate Cancer Treatment
- PMID: 38261043
- PMCID: PMC10807259
- DOI: 10.1001/jama.2023.26491
Functional Outcomes After Localized Prostate Cancer Treatment
Abstract
Importance: Adverse outcomes associated with treatments for localized prostate cancer remain unclear.
Objective: To compare rates of adverse functional outcomes between specific treatments for localized prostate cancer.
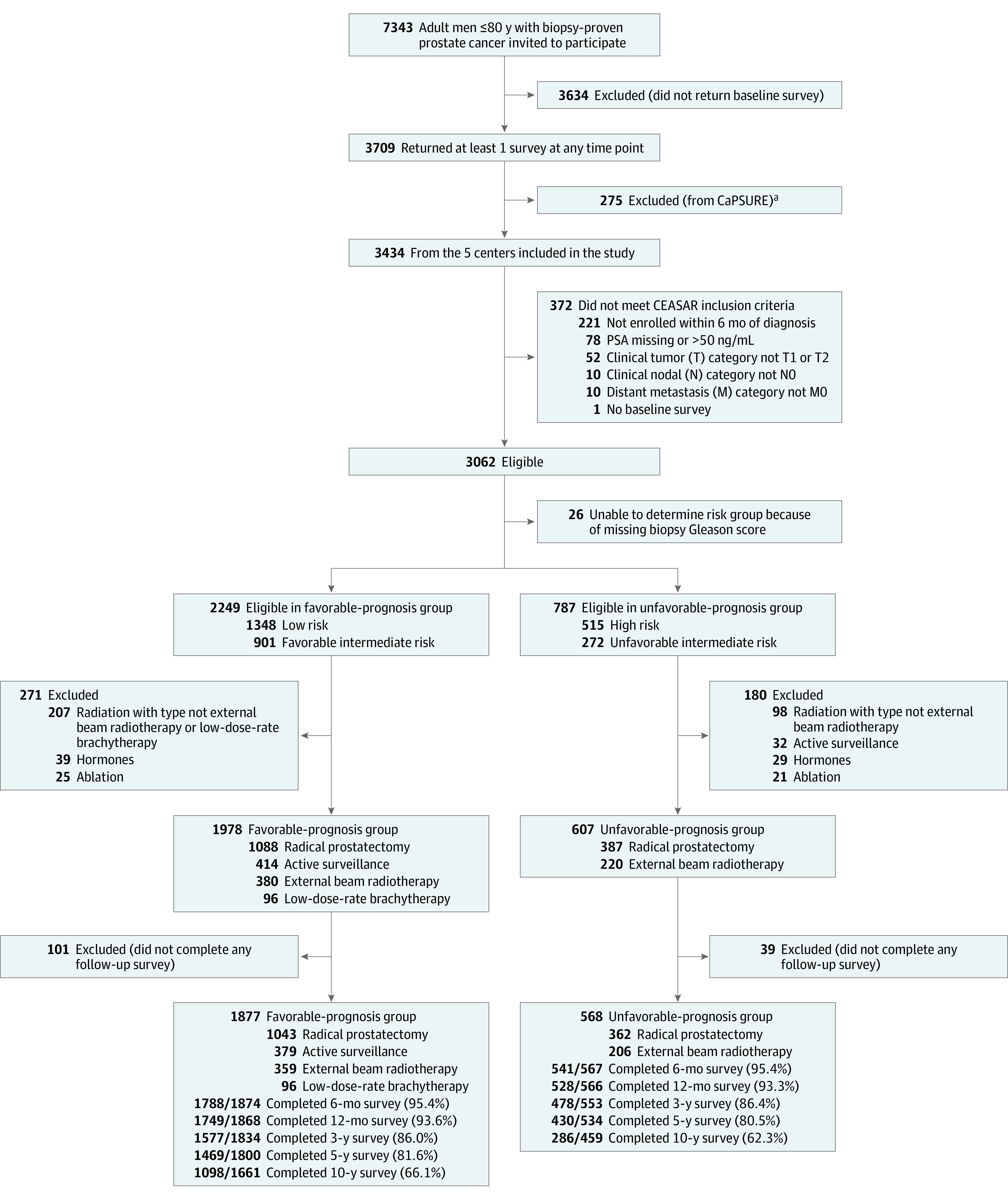
Design, setting, and participants: An observational cohort study using data from 5 US Surveillance, Epidemiology, and End Results Program registries. Participants were treated for localized prostate cancer between 2011 and 2012. At baseline, 1877 had favorable-prognosis prostate cancer (defined as cT1-cT2bN0M0, prostate-specific antigen level <20 ng/mL, and grade group 1-2) and 568 had unfavorable-prognosis prostate cancer (defined as cT2cN0M0, prostate-specific antigen level of 20-50 ng/mL, or grade group 3-5). Follow-up data were collected by questionnaire through February 1, 2022.
Exposures: Radical prostatectomy (n = 1043), external beam radiotherapy (n = 359), brachytherapy (n = 96), or active surveillance (n = 379) for favorable-prognosis disease and radical prostatectomy (n = 362) or external beam radiotherapy with androgen deprivation therapy (n = 206) for unfavorable-prognosis disease.
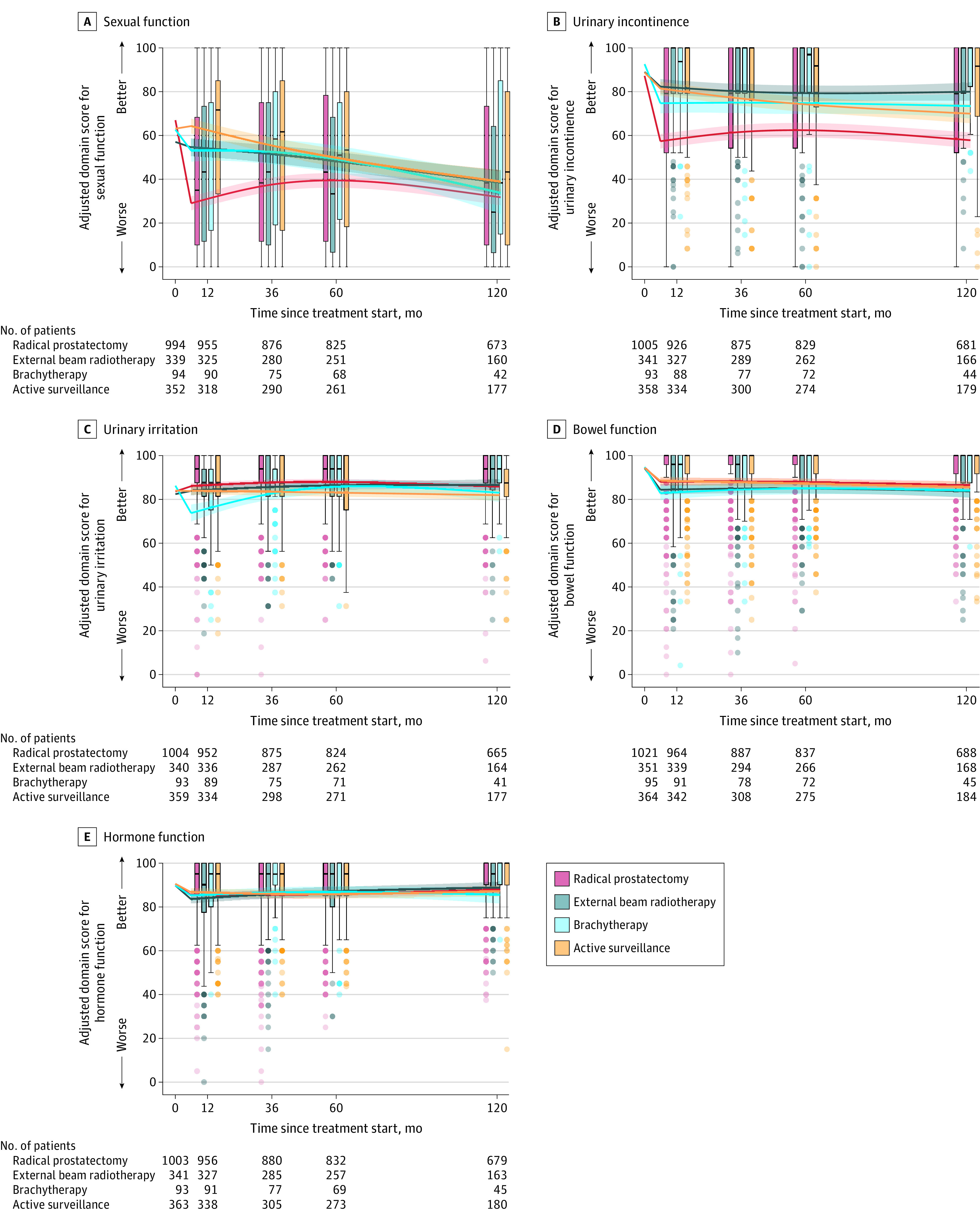
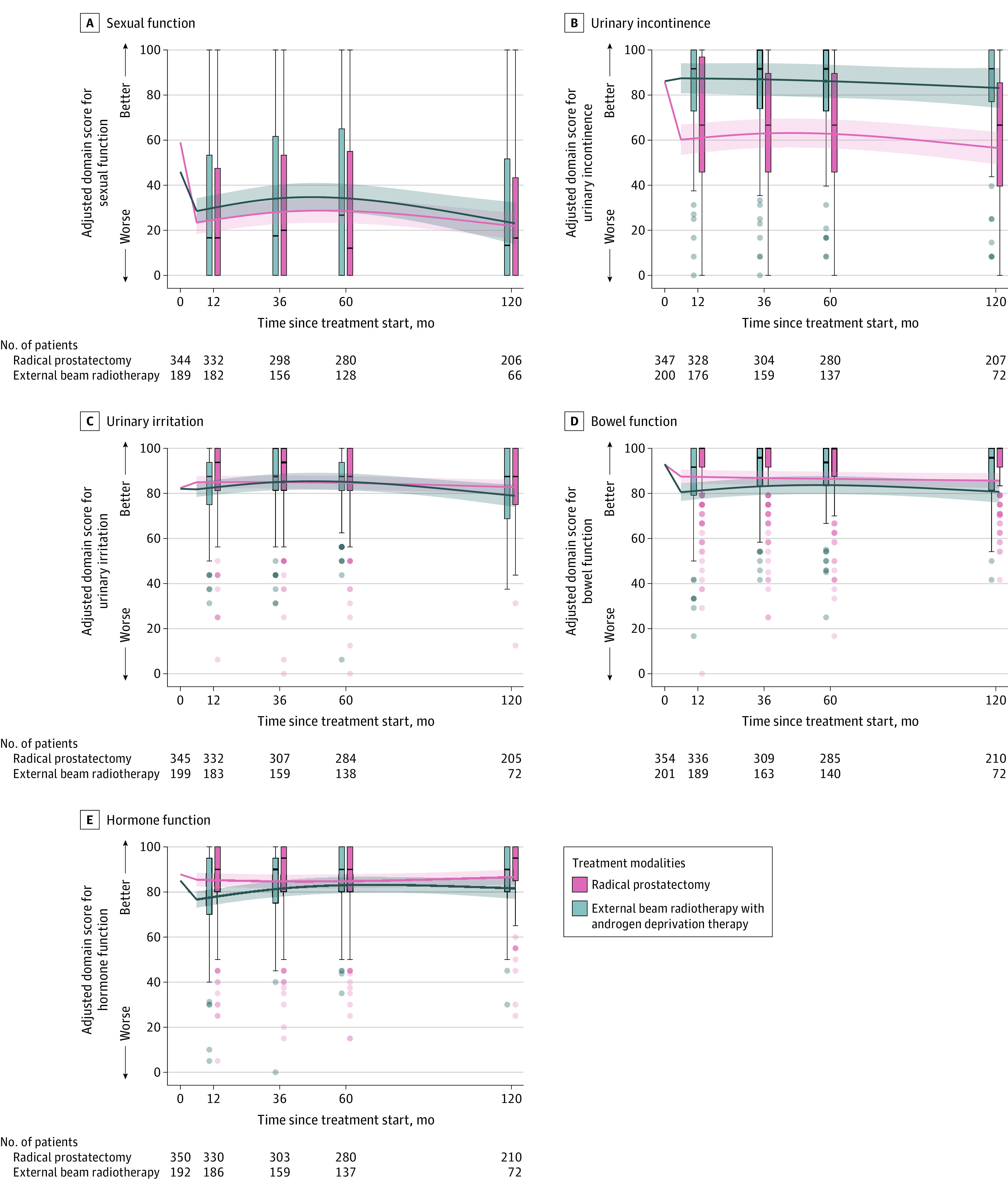
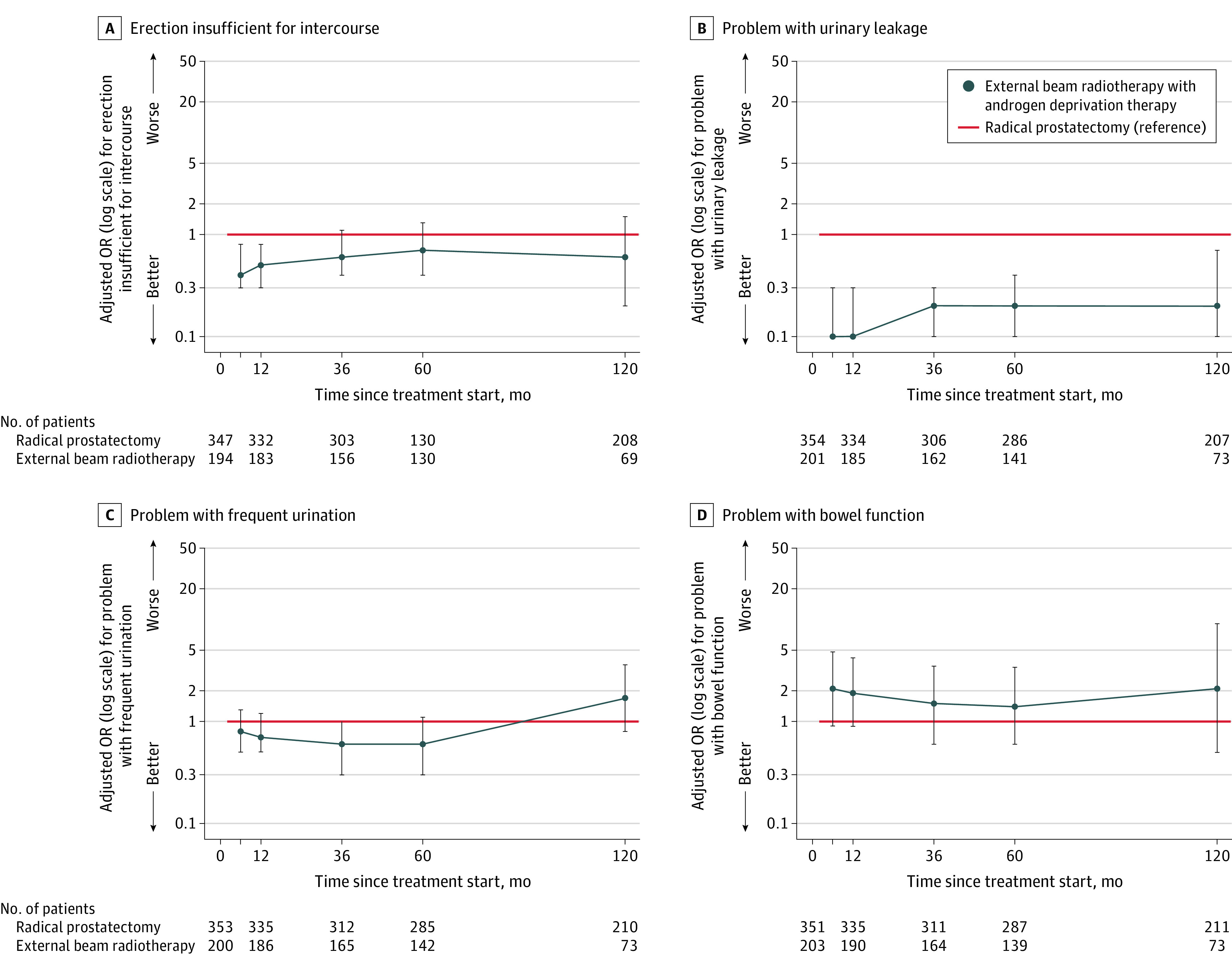
Main outcomes and measures: Outcomes were patient-reported sexual, urinary, bowel, and hormone function measured using the 26-item Expanded Prostate Cancer Index Composite (range, 0-100; 100 = best). Associations of specific therapies with each outcome were estimated and compared at 10 years after treatment, adjusting for corresponding baseline scores, and patient and tumor characteristics. Minimum clinically important differences were 10 to 12 for sexual function, 6 to 9 for urinary incontinence, 5 to 7 for urinary irritation, and 4 to 6 for bowel and hormone function.
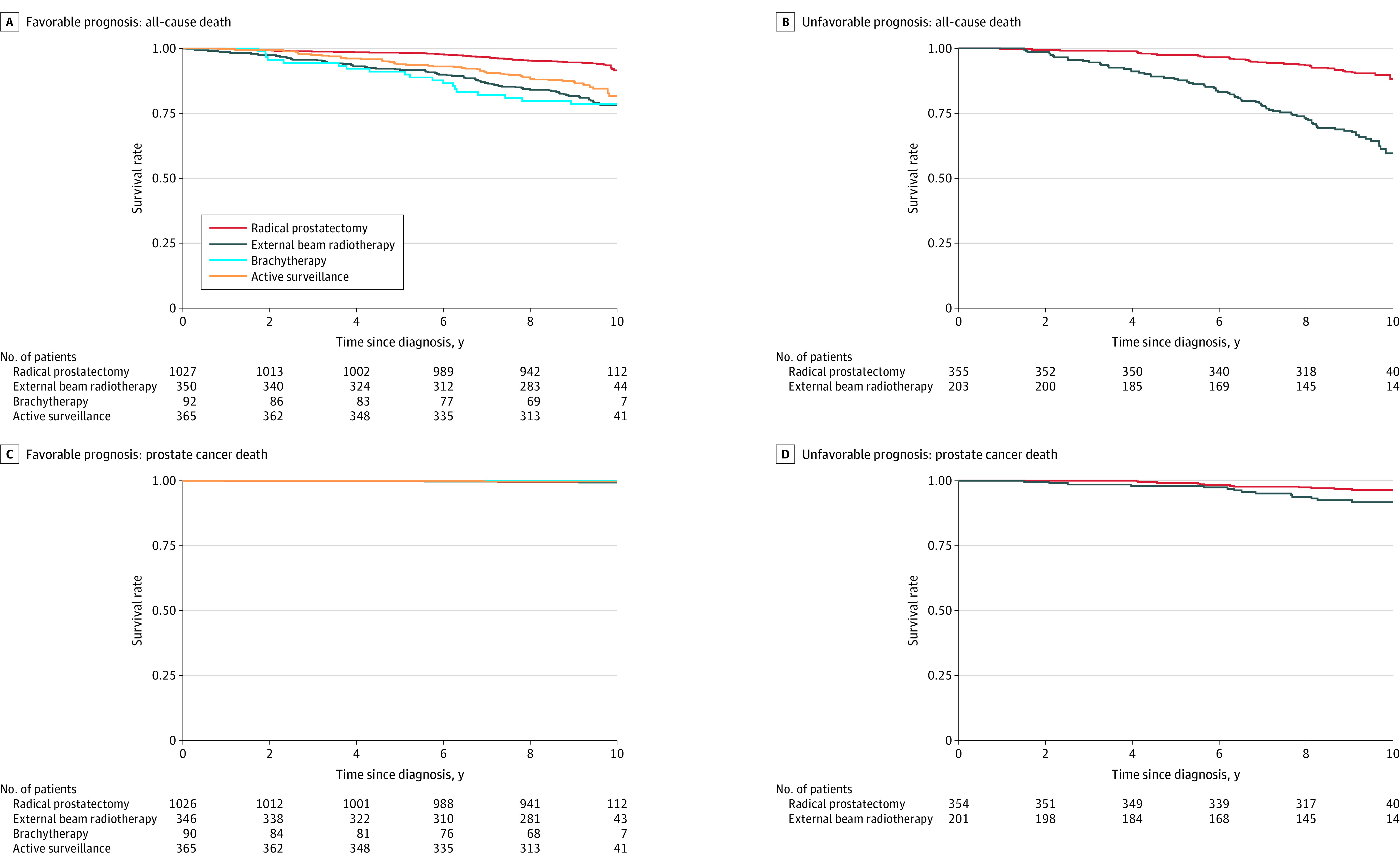
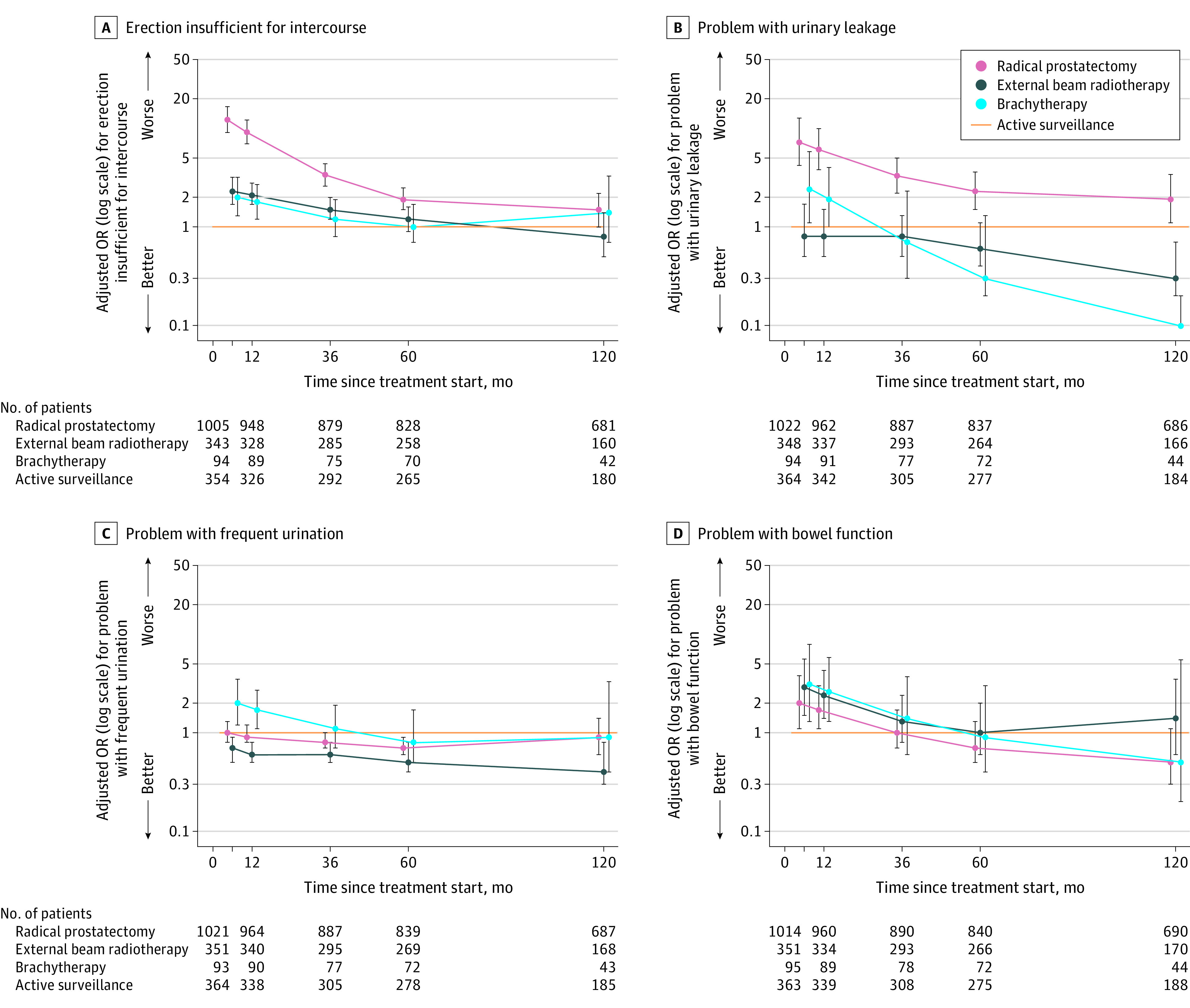
Results: A total of 2445 patients with localized prostate cancer (median age, 64 years; 14% Black, 8% Hispanic) were included and followed up for a median of 9.5 years. Among 1877 patients with favorable prognosis, radical prostatectomy was associated with worse urinary incontinence (adjusted mean difference, -12.1 [95% CI, -16.2 to -8.0]), but not worse sexual function (adjusted mean difference, -7.2 [95% CI, -12.3 to -2.0]), compared with active surveillance. Among 568 patients with unfavorable prognosis, radical prostatectomy was associated with worse urinary incontinence (adjusted mean difference, -26.6 [95% CI, -35.0 to -18.2]), but not worse sexual function (adjusted mean difference, -1.4 [95% CI, -11.1 to 8.3), compared with external beam radiotherapy with androgen deprivation therapy. Among patients with unfavorable prognosis, external beam radiotherapy with androgen deprivation therapy was associated with worse bowel (adjusted mean difference, -4.9 [95% CI, -9.2 to -0.7]) and hormone (adjusted mean difference, -4.9 [95% CI, -9.5 to -0.3]) function compared with radical prostatectomy.
Conclusions and relevance: Among patients treated for localized prostate cancer, radical prostatectomy was associated with worse urinary incontinence but not worse sexual function at 10-year follow-up compared with radiotherapy or surveillance among people with more favorable prognosis and compared with radiotherapy for those with unfavorable prognosis. Among men with unfavorable-prognosis disease, external beam radiotherapy with androgen deprivation therapy was associated with worse bowel and hormone function at 10-year follow-up compared with radical prostatectomy.
Conflict of interest statement
Figures
Comment in
-
Outcomes Following Localized Prostate Cancer Treatment.JAMA. 2024 May 28;331(20):1769-1770. doi: 10.1001/jama.2024.5489. JAMA. 2024. PMID: 38683554 No abstract available.
-
Outcomes Following Localized Prostate Cancer Treatment.JAMA. 2024 May 28;331(20):1769. doi: 10.1001/jama.2024.5486. JAMA. 2024. PMID: 38683568 No abstract available.
References
-
- Hoffman KE, Penson DF, Zhao Z, et al. Patient-reported outcomes through 5 years for active surveillance, surgery, brachytherapy, or external beam radiation with or without androgen deprivation therapy for localized prostate cancer. JAMA. 2020;323(2):149-163. doi: 10.1001/jama.2019.20675 - DOI - PMC - PubMed
-
- Chen RC, Basak R, Meyer AM, et al. Association between choice of radical prostatectomy, external beam radiotherapy, brachytherapy, or active surveillance and patient-reported quality of life among men with localized prostate cancer. JAMA. 2017;317(11):1141-1150. doi: 10.1001/jama.2017.1652 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
