

Cancer Diagnoses After Recent Weight Loss
- PMID: 38261044
- PMCID: PMC10807298
- DOI: 10.1001/jama.2023.25869
Cancer Diagnoses After Recent Weight Loss
Abstract
Importance: Weight loss is common in primary care. Among individuals with recent weight loss, the rates of cancer during the subsequent 12 months are unclear compared with those without recent weight loss.
Objective: To determine the rates of subsequent cancer diagnoses over 12 months among health professionals with weight loss during the prior 2 years compared with those without recent weight loss.
Design, setting, and participants: Prospective cohort analysis of females aged 40 years or older from the Nurses' Health Study who were followed up from June 1978 until June 30, 2016, and males aged 40 years or older from the Health Professionals Follow-Up Study who were followed up from January 1988 until January 31, 2016.
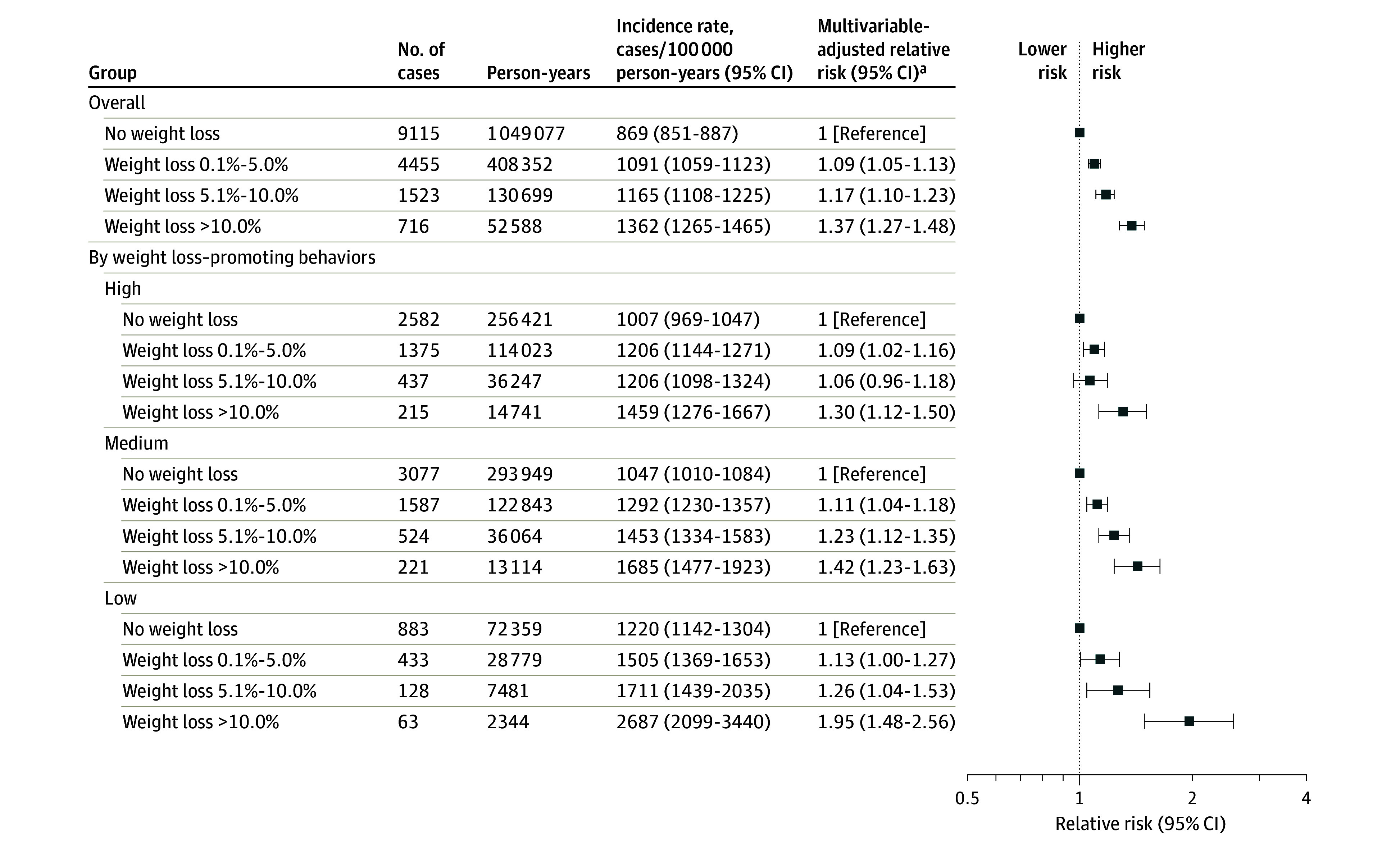
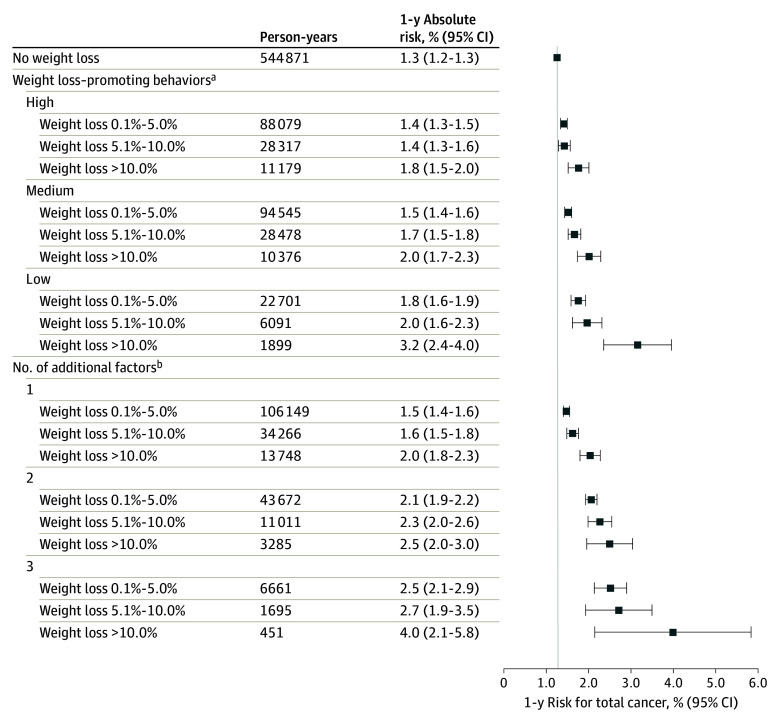
Exposure: Recent weight change was calculated from the participant weights that were reported biennially. The intentionality of weight loss was categorized as high if both physical activity and diet quality increased, medium if only 1 increased, and low if neither increased.
Main outcome and measures: Rates of cancer diagnosis during the 12 months after weight loss.
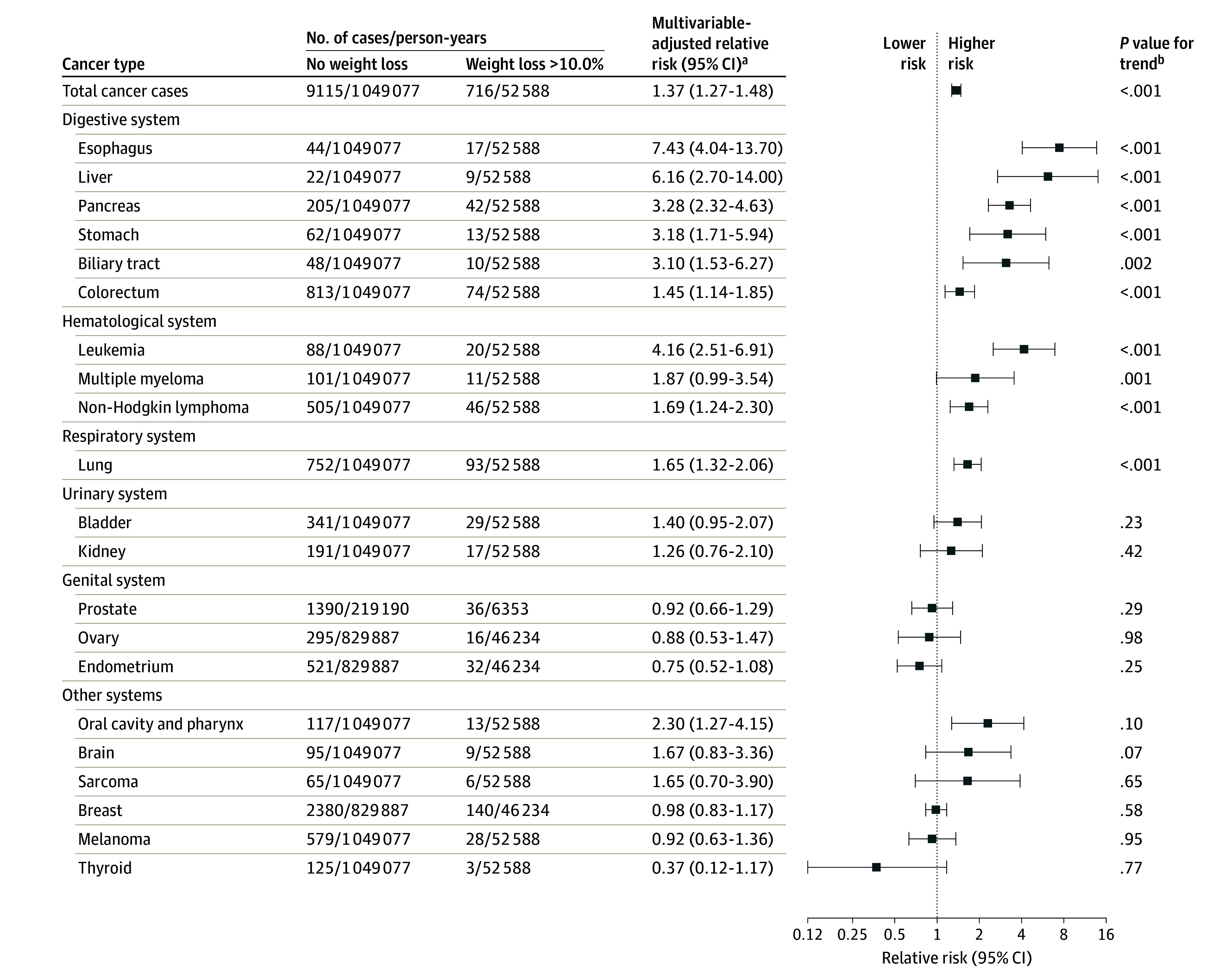
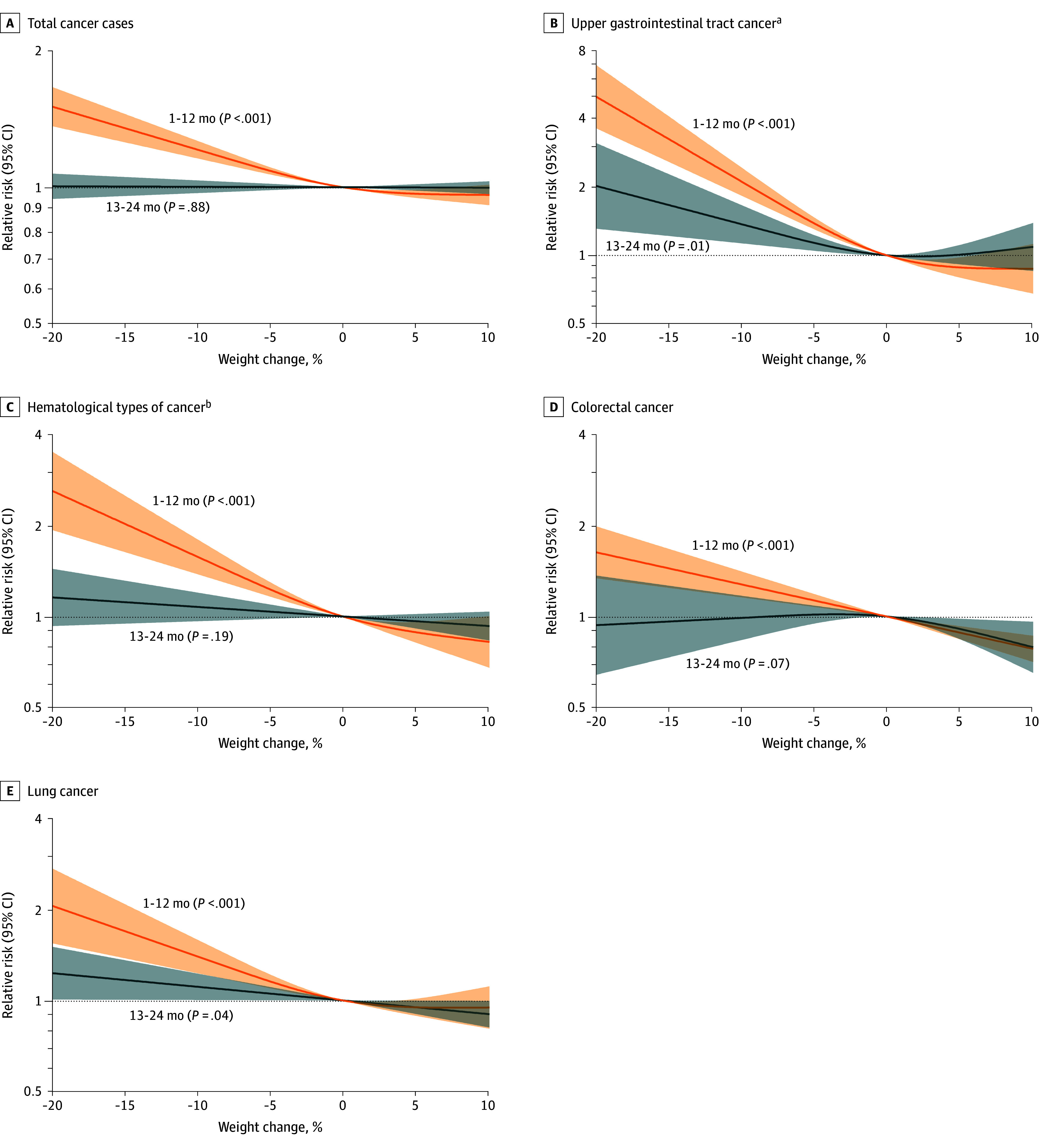
Results: Among 157 474 participants (median age, 62 years [IQR, 54-70 years]; 111 912 were female [71.1%]; there were 2631 participants [1.7%] who self-identified as Asian, Native American, or Native Hawaiian; 2678 Black participants [1.7%]; and 149 903 White participants [95.2%]) and during 1.64 million person-years of follow-up, 15 809 incident cancer cases were identified (incident rate, 964 cases/100 000 person-years). During the 12 months after reported weight change, there were 1362 cancer cases/100 000 person-years among all participants with recent weight loss of greater than 10.0% of body weight compared with 869 cancer cases/100 000 person-years among those without recent weight loss (between-group difference, 493 cases/100 000 person-years [95% CI, 391-594 cases/100 000 person-years]; P < .001). Among participants categorized with low intentionality for weight loss, there were 2687 cancer cases/100 000 person-years for those with weight loss of greater than 10.0% of body weight compared with 1220 cancer cases/100 000 person-years for those without recent weight loss (between-group difference, 1467 cases/100 000 person-years [95% CI, 799-2135 cases/100 000 person-years]; P < .001). Cancer of the upper gastrointestinal tract (cancer of the esophagus, stomach, liver, biliary tract, or pancreas) was particularly common among participants with recent weight loss; there were 173 cancer cases/100 000 person-years for those with weight loss of greater than 10.0% of body weight compared with 36 cancer cases/100 000 person-years for those without recent weight loss (between-group difference, 137 cases/100 000 person-years [95% CI, 101-172 cases/100 000 person-years]; P < .001).
Conclusions and relevance: Health professionals with weight loss within the prior 2 years had a significantly higher risk of cancer during the subsequent 12 months compared with those without recent weight loss. Cancer of the upper gastrointestinal tract was particularly common among participants with recent weight loss compared with those without recent weight loss.
Conflict of interest statement
Figures
Comment in
-
Diagnosis of Cancer After Recent Weight Loss.JAMA. 2024 May 21;331(19):1678. doi: 10.1001/jama.2024.5416. JAMA. 2024. PMID: 38656761 No abstract available.
