

Right ventricular injury in critically ill patients with COVID-19: a descriptive study with standardized echocardiographic follow-up
- PMID: 38261092
- PMCID: PMC10805901
- DOI: 10.1186/s13613-024-01248-8
Right ventricular injury in critically ill patients with COVID-19: a descriptive study with standardized echocardiographic follow-up
Abstract
Purpose: Patients with COVID-19 admitted to intensive care unit (ICU) may have right ventricular (RV) injury. The main goal of this study was to investigate the incidence of RV injury and to describe the patient trajectories in terms of RV injury during ICU stay.
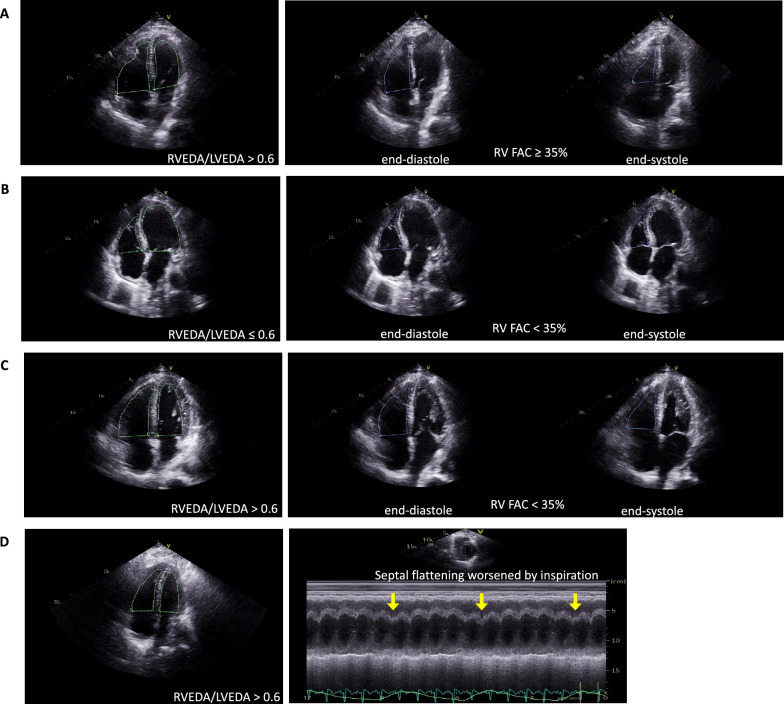
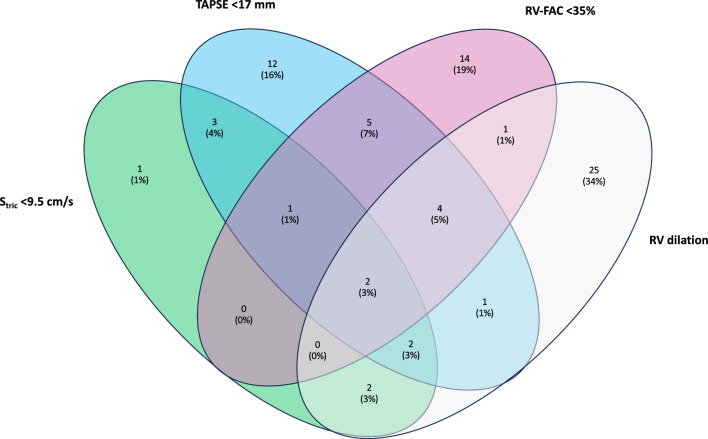
Methods: Prospective and bicentric study with standardized transthoracic echocardiographic (TTE) follow-up during ICU stay with a maximum follow-up of 28 days. The different patterns of RV injury were isolated RV dilation, RV dysfunction (tricuspid annular plane systolic excursion < 17 mm and/or systolic tricuspid annular velocity < 9.5 cm/s and/or RV fractional area change < 35%) without RV dilation, RV dysfunction with RV dilation and acute cor pulmonale (ACP, RV dilatation with paradoxical septal motion). The different RV injury patterns were described and their association with Day-28 mortality was investigated.
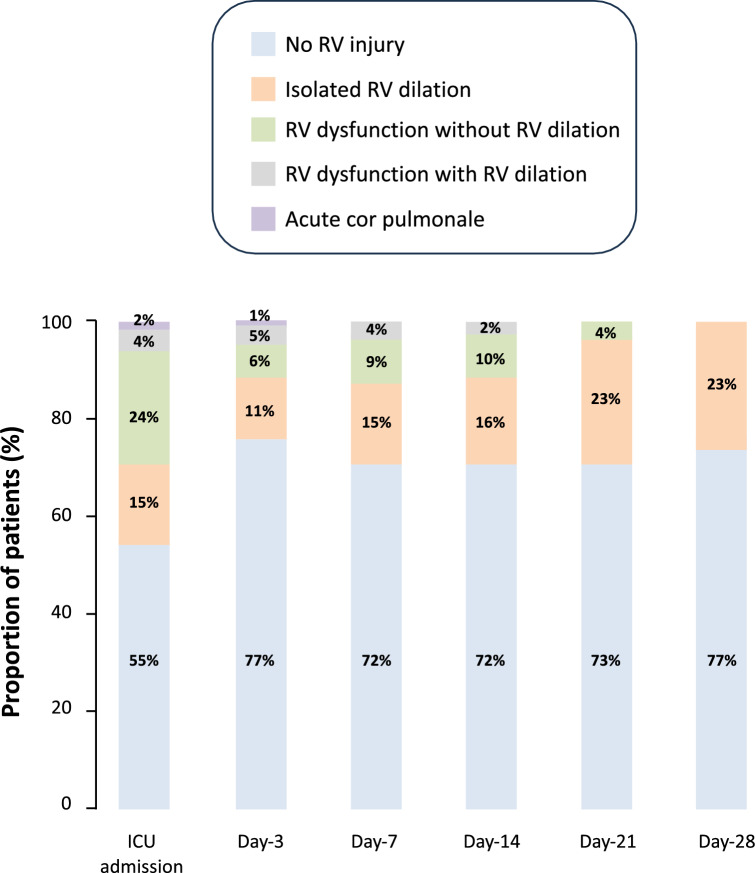
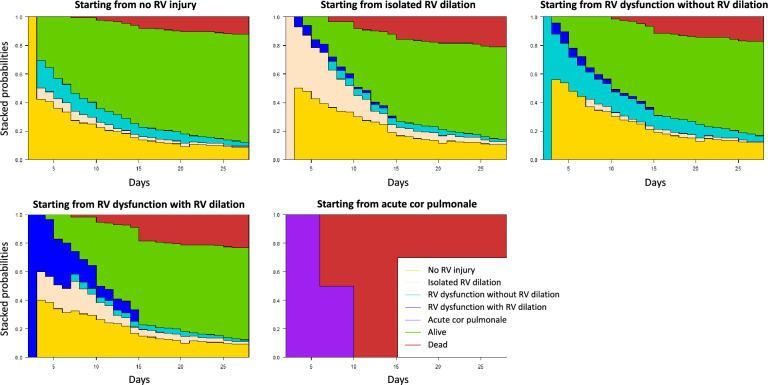
Results: Of 118 patients with complete echocardiographic follow-up who underwent 393 TTE examinations during ICU stay, 73(62%) had at least one RV injury pattern during one or several TTE examinations: 29(40%) had isolated RV dilation, 39(53%) had RV dysfunction without RV dilation, 10(14%) had RV dysfunction with RV dilation and 2(3%) had ACP. Patients with RV injury were more likely to have cardiovascular risk factors, to be intubated and to receive norepinephrine and had a higher Day-28 mortality rate (27 vs. 7%, p < 0.01). RV injury was isolated in 82% of cases, combined with left ventricular systolic dysfunction in 18% of cases and 10% of patients with RV injury experienced several patterns of RV injury during ICU stay. The number of patients with de novo RV injury decreased over time, no patient developed de novo RV injury after Day-14 regardless of the RV injury pattern and 20(31%) patients without RV injury on ICU admission developed RV injury during ICU stay. Only the combination of RV dysfunction with RV dilation or ACP (aHR = 3.18 95% CI(1.16-8.74), p = 0.03) was associated with Day-28 mortality.
Conclusion: RV injury was frequent in COVID-19 patients, occurred within the first two weeks after ICU admission and was most often isolated. Only the combination of RV dysfunction with RV dilation or ACP could potentially be associated with Day-28 mortality. Clinical trial registration NCT04335162.
Keywords: Acute respiratory distress syndrome; COVID-19; Cardiac injury; Prognosis; Right ventricle.
© 2024. The Author(s).
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
-
- Jansson S, Blixt PJ, Didriksson H, Jonsson C, Andersson H, Hedstrom C, et al. Incidence of acute myocardial injury and its association with left and right ventricular systolic dysfunction in critically ill COVID-19 patients. Ann Intensive Care. 2022;12(1):56. doi: 10.1186/s13613-022-01030-8. - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
