

Comparing three-dimensional and two-dimensional deep-learning, radiomics, and fusion models for predicting occult lymph node metastasis in laryngeal squamous cell carcinoma based on CT imaging: a multicentre, retrospective, diagnostic study
- PMID: 38261897
- PMCID: PMC10796944
- DOI: 10.1016/j.eclinm.2023.102385
Comparing three-dimensional and two-dimensional deep-learning, radiomics, and fusion models for predicting occult lymph node metastasis in laryngeal squamous cell carcinoma based on CT imaging: a multicentre, retrospective, diagnostic study
Abstract
Background: The occult lymph node metastasis (LNM) of laryngeal squamous cell carcinoma (LSCC) affects the treatment and prognosis of patients. This study aimed to comprehensively compare the performance of the three-dimensional and two-dimensional deep learning models, radiomics model, and the fusion models for predicting occult LNM in LSCC.
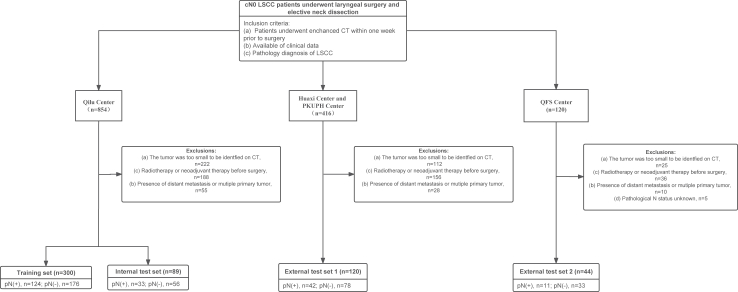
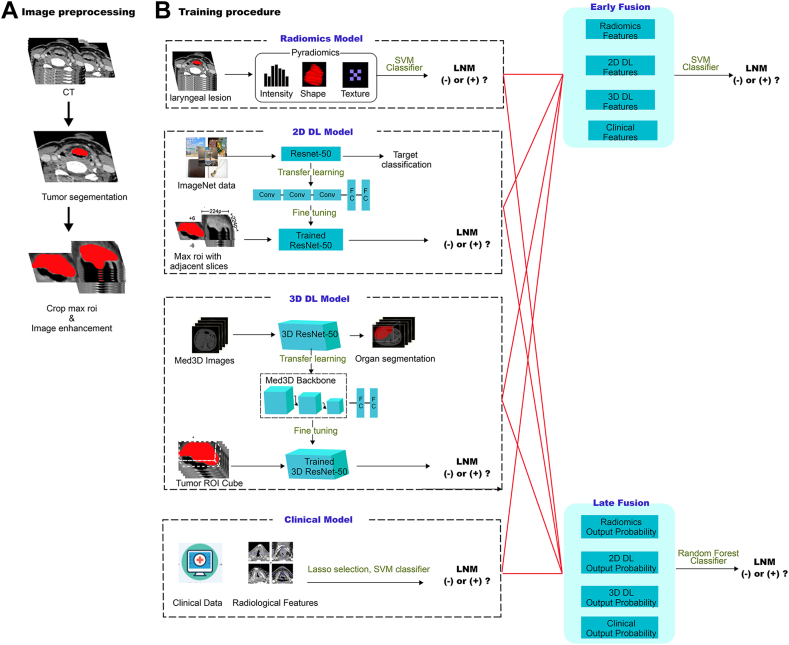
Methods: In this retrospective diagnostic study, a total of 553 patients with clinical N0 stage LSCC, who underwent surgical treatment without distant metastasis and multiple primary cancers, were consecutively enrolled from four Chinese medical centres between January 01, 2016 and December 30, 2020. The participant data were manually retrieved from medical records, imaging databases, and pathology reports. The study cohort was divided into a training set (n = 300), an internal test set (n = 89), and two external test sets (n = 120 and 44, respectively). The three-dimensional deep learning (3D DL), two-dimensional deep learning (2D DL), and radiomics model were developed using CT images of the primary tumor. The clinical model was constructed based on clinical and radiological features. Two fusion strategies were utilized to develop the fusion model: the feature-based DLRad_FB model and the decision-based DLRad_DB model. The discriminative ability and correlation of 3D DL, 2D DL and radiomics features were analysed comprehensively. The performances of the predictive models were evaluated based on the pathological diagnosis.
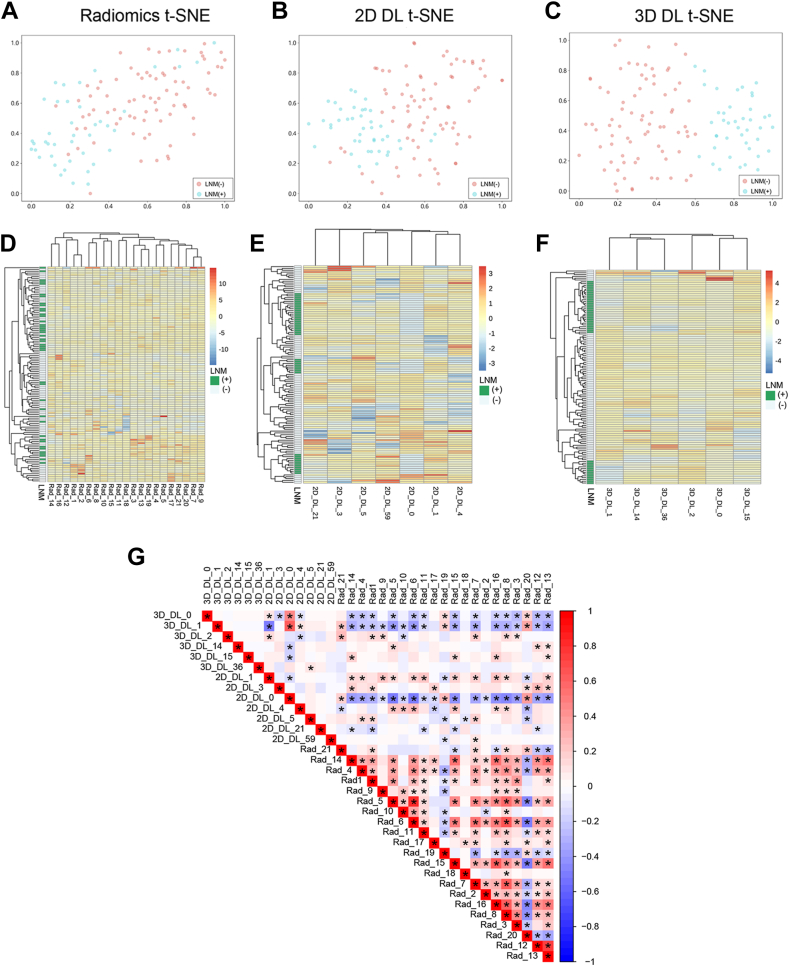
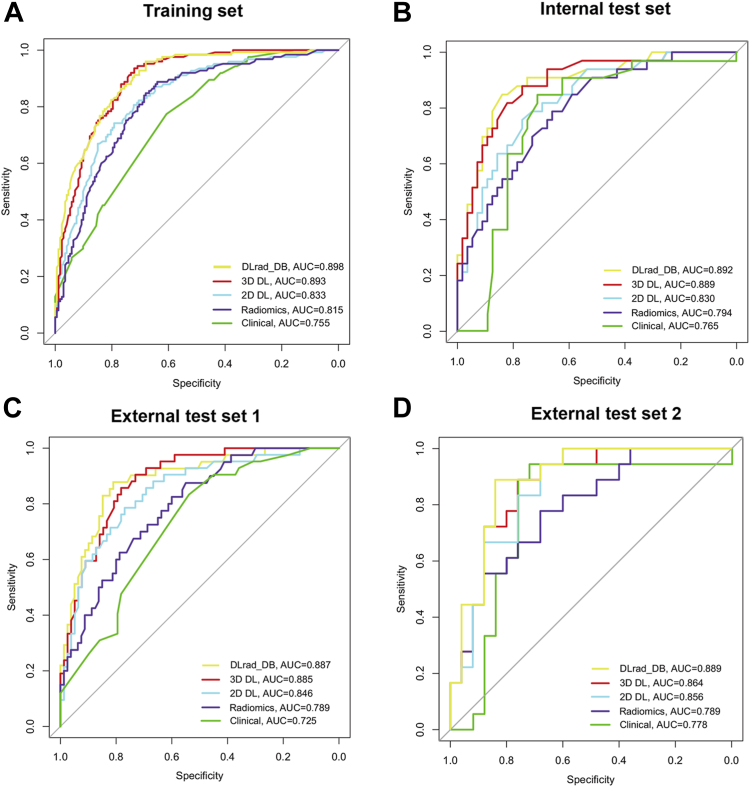
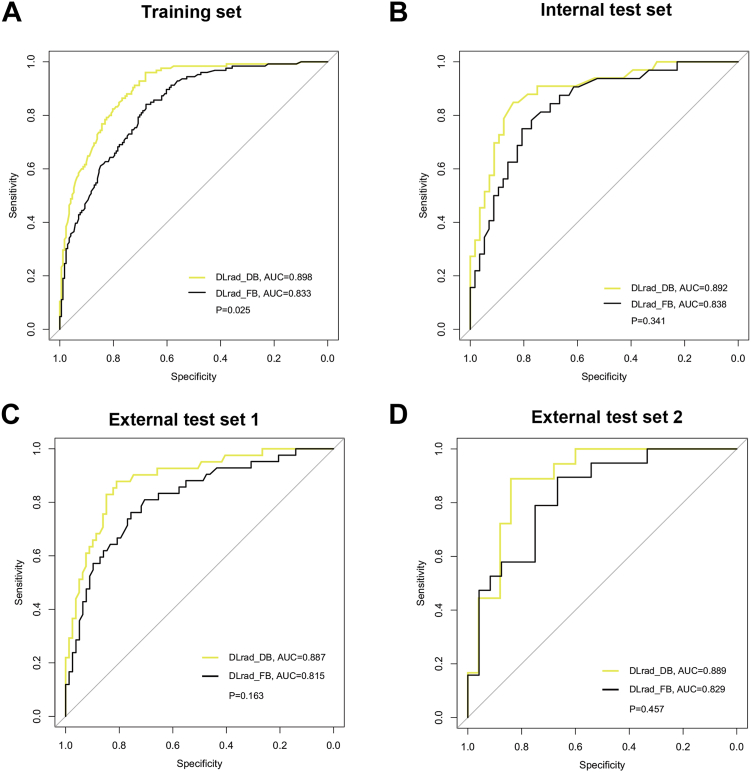
Findings: The 3D DL features had superior discriminative ability and lower internal redundancy compared to 2D DL and radiomics features. The DLRad_DB model achieved the highest AUC (0.89-0.90) among all the study sets, significantly outperforming the clinical model (AUC = 0.73-0.78, P = 0.0001-0.042, Delong test). Compared to the DLRad_DB model, the AUC values for the DLRad_FB, 3D DL, 2D DL, and radiomics models were 0.82-0.84 (P = 0.025-0.46), 0.86-0.89 (P = 0.75-0.97), 0.83-0.86 (P = 0.029-0.66), and 0.79-0.82 (P = 0.0072-0.10), respectively in the study sets. Additionally, the DLRad_DB model exhibited the best sensitivity (82-88%) and specificity (79-85%) in the test sets.
Interpretation: The decision-based fusion model DLRad_DB, which combines 3D DL, 2D DL, radiomics, and clinical data, can be utilized to predict occult LNM in LSCC. This has the potential to minimize unnecessary lymph node dissection and prophylactic radiotherapy in patients with cN0 disease.
Funding: National Natural Science Foundation of China, Natural Science Foundation of Shandong Province.
Keywords: Artificial intelligence; Deep learning; Laryngeal cancer; Occult lymph node metastasis; Radiomics.
© 2023 The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures
References
-
- Steuer C.E., El-Deiry M., Parks J.R., Higgins K.A., Saba N.F. An update on larynx cancer. CA Cancer J Clin. 2017;67(1):31–50. - PubMed
-
- Siegel R.L., Miller K.D., Wagle N.S., Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. - PubMed
-
- Sharbel D.D., Abkemeier M., Groves M.W., Albergotti W.G., Byrd J.K., Reyes-Gelves C. Occult metastasis in laryngeal squamous cell carcinoma: a systematic review and meta-analysis. Ann Otol Rhinol Laryngol. 2021;130(1):67–77. - PubMed
-
- Saito Y., Yoshimoto S., Kitayama M., et al. Elective neck dissection for T3-T4N0 laryngeal carcinoma: evidence from Japan's National Head and Neck Cancer Registry. Int J Clin Oncol. 2023;28(2):209–220. - PubMed
-
- Petrarolha S., Dedivitis R., Matos L., Ramos D., Kulcsar M. Lymph node density as a predictive factor for worse outcomes in laryngeal cancer. Eur Arch Otorhinolaryngol. 2020;277(3):833–840. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
