

Poor Glycemic Control Is Associated With More Rapid Kidney Function Decline After the Onset of Diabetic Kidney Disease
- PMID: 38262002
- PMCID: PMC11244193
- DOI: 10.1210/clinem/dgae044
Poor Glycemic Control Is Associated With More Rapid Kidney Function Decline After the Onset of Diabetic Kidney Disease
Abstract
Background: The role of glycemic control and its variability on the rate of kidney function decline after the onset of diabetic kidney disease (DKD) remains unclear.
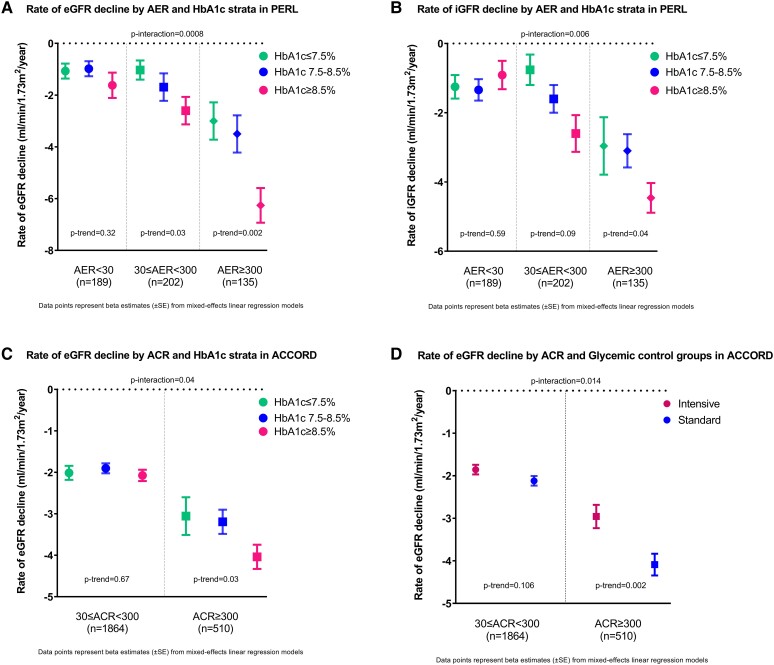
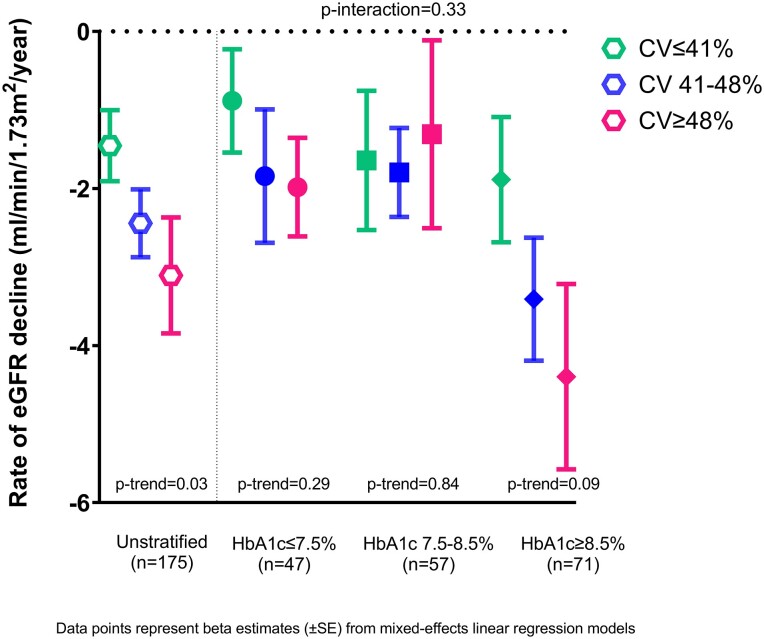
Methods: The association between baseline glycated hemoglobin (HbA1c) and rates of estimated glomerular filtration rate (eGFR) loss during follow-up was examined by mixed-effects linear regression in 530 individuals with type 1 diabetes and early-to-moderate DKD from the Preventing Early Renal Loss (PERL) trial and 2378 individuals with type 2 diabetes and established DKD from the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. The benefit of intensive vs standard glycemic control in slowing eGFR decline was examined in ACCORD. The associations between continuous glucose monitoring-derived short-term glycemic variability indices and rate of eGFR decline were also evaluated in PERL.
Results: A higher baseline HbA1c was associated with a more negative eGFR slope in both PERL and ACCORD (-0.87 and -0.27 mL/min/1.73 m2/year per Hba1c unit increment, P < .0001 and P = .0002, respectively). In both studies, the strength of this association progressively increased with increasing levels of albuminuria (P for interaction <.05). Consistent with this, the benefit of intensive glycemic control on eGFR decline was greater in ACCORD participants with severe rather than moderate albuminuria (+1.13 vs + 0.26 mL/min/1.73 m2/year, P = .01). No independent associations were found in PERL between short-term glycemic variability indices and rate of eGFR decline.
Conclusion: In both type 1 and type 2 diabetes, poor glycemic control is associated with a more rapid rate of glomerular filtration rate decline after DKD onset, especially in persons with severe albuminuria.
Keywords: diabetic kidney disease; glycemic control; kidney function decline.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- United States Renal Data System . 2022 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. 2022. https://adr.usrds.org/2022 - PMC - PubMed
-
- Gregg EW, Zhuo X, Cheng YJ, Albright AL, Narayan KM, Thompson TJ. Trends in lifetime risk and years of life lost due to diabetes in the USA, 1985-2011: a modelling study. Lancet Diabetes Endocrinol. 2014;2(11):867‐874. - PubMed
-
- Effect of intensive therapy on the development and progression of diabetic nephropathy in the Diabetes Control and Complications Trial. The Diabetes Control and Complications (DCCT) Research Group. Kidney Int. 1995;47(6):1703‐1720. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- General Clinical Research Centers and Clinical and Translational Science Awards
- UL1-TR-002494/TR/NCATS NIH HHS/United States
- Washington University DRC
- 17-2012-377/JDRF/United States
- P30 AG024824/AG/NIA NIH HHS/United States
- 2018PG-TlD014/Helmsley Charitable Trust
- N01-HC-95178/HL/NHLBI NIH HHS/United States
- P30 DK020572/DK/NIDDK NIH HHS/United States
- #NNF OC0013659/Novo Nordisk Foundation
- R01-DK-126373/NH/NIH HHS/United States
- CC/CDC HHS/United States
- Y01 HC001010/HC/NHLBI NIH HHS/United States
- UL1 TR001105/TR/NCATS NIH HHS/United States
- EY/NEI NIH HHS/United States
- P30-AG-024824/AG/NIA NIH HHS/United States
- R03-DK-094484/DK/NIDDK NIH HHS/United States
- P30 DK036836/DK/NIDDK NIH HHS/United States
- R01 DK126373/DK/NIDDK NIH HHS/United States
- P30 DK020579/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
