

Preventive treatment patterns in the adult migraine population: an observational UK study over 7 years
- PMID: 38262999
- PMCID: PMC10807158
- DOI: 10.1186/s12875-023-02242-y
Preventive treatment patterns in the adult migraine population: an observational UK study over 7 years
Abstract
Background: Calcitonin gene-related peptide monoclonal antibodies (CGRP mAbs) are recommended by the United Kingdom National Institute of Health and Care Excellence for the prevention of migraine as treatment beyond third line. We report migraine prevalence and preventive treatment patterns in the adult United Kingdom primary care population over a 7.5-year period, focusing on patients ceasing ≥ 3 oral preventive medication classes.
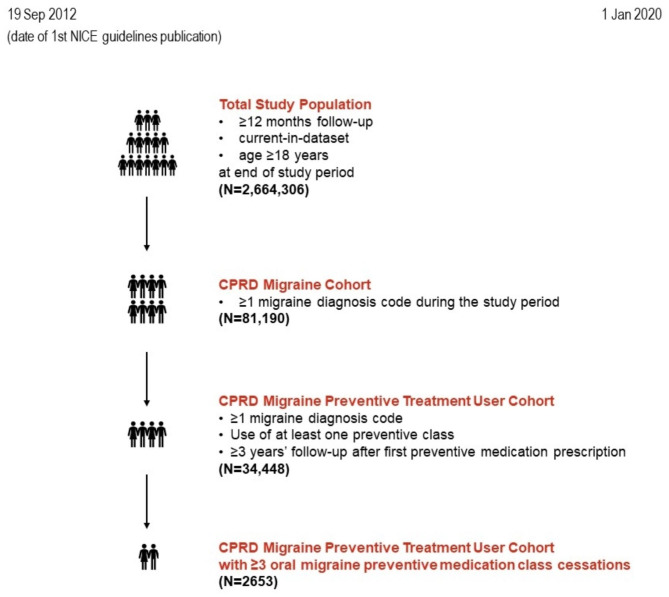
Methods: Study populations were retrieved from the Clinical Practice Research Datalink GOLD database (study period: 19 September 2012 to 1 January 2020; inclusion criteria: ≥12 months follow-up, current-in-dataset, adult on 1 January 2020). Patients who used ≥ 1 oral preventive medication with ≥ 3-year follow-up after first prescription were considered preventive treatment users; class cessation was defined as cessation without evidence of restart within 6 months from end-of-supply date.
Results: On 1 January 2020, 3.0% of the total study population were diagnosed with migraine (n = 81,190/2,664,306); of these, 42.4% were preventive treatment users (n = 34,448/81,190). The most frequently used oral migraine preventive medication classes were beta-blockers (n = 14,713), tricyclic antidepressants (n = 14,415) and antiepileptics (n = 6497). Among preventive treatment users, 7.7% (n = 2653/34,448) ceased ≥ 3 oral preventive medication classes; of these, 21.7% (n = 576/2653) had been referred to a neurologist.
Conclusions: Compared to existing population-based estimates of migraine prevalence, our data further corroborates that a considerable proportion of patients with migraine do not seek treatment. Among those who sought primary care within a 7.5-year period, almost half received empirical oral preventive treatment. Importantly, nearly 1 of 10 preventive treatment users ceased ≥ 3 oral preventive medication classes, highlighting a need for additional therapeutic options. These patients may benefit from CGRP antagonists and/or injectable onabotulinumtoxinA; however, only a minority was referred to specialist care, where these options would be more available.
Trial registration: Not applicable.
Keywords: CPRD; Calcitonin gene-related peptide antagonists; Migraine epidemiology; Migraine preventive medications.
© 2024. The Author(s).
Conflict of interest statement
Nazanin Kondori, Andrew Pain, Julie Mount, Camilla Appel, Michael Ranopa and Tania Gulati are employees of Eli Lilly and Company. David Kernick declares advisory and education work for Allergan, Eli Lilly and Company, Novartis, Pfizer and Teva.
Figures


References
-
- Warshaw LJ, Burton WN, Silberstein SD, et al. Migraine: a problem for employers and managed care plans. Am J Manag Care. 1997;3:1515–23. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials