

Classifications of anterior segment structure of congenital corneal opacity in infants and toddlers by ultrasound biomicroscopy and slit-lamp microscopic photographs: an observational study
- PMID: 38263030
- PMCID: PMC10804776
- DOI: 10.1186/s12886-024-03286-z
Classifications of anterior segment structure of congenital corneal opacity in infants and toddlers by ultrasound biomicroscopy and slit-lamp microscopic photographs: an observational study
Abstract
Background: The structural features have an impact on the surgical prognosis for congenital corneal opacity (CCO). The structural classification system of CCO, however, is lacking. Based on data from ultrasound biomicroscopy (UBM) findings in infants and toddlers with CCO, this research proposed a classification system for the anterior segment structure severity.
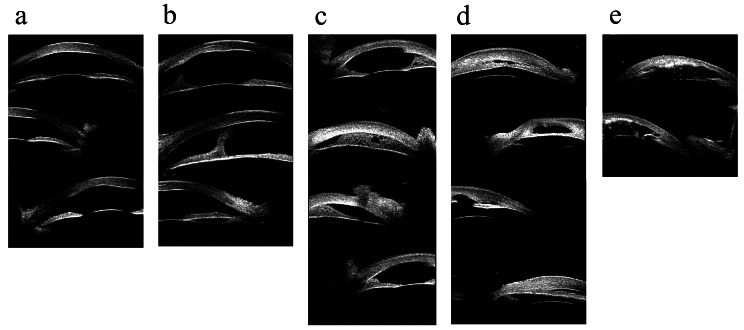
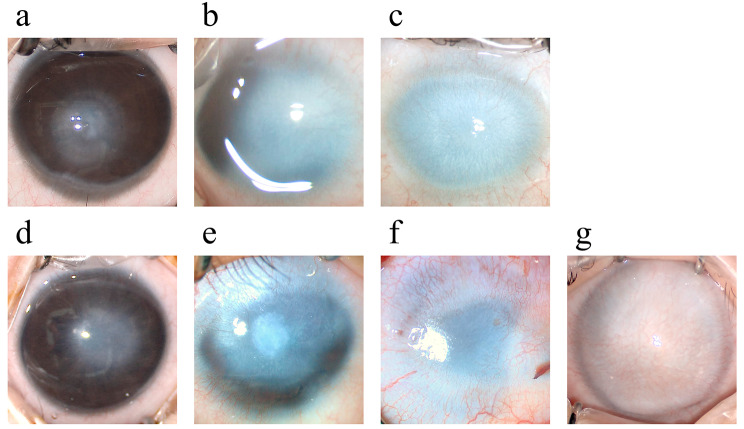
Methods: Medical records, preoperative UBM images and slit-lamp photographs of infants and toddlers diagnosed with CCO at University Third Hospital between December 2018 and June 2022 were reviewed. According to the anterior segment structural features observed in UBM images, eyes were classified as follows: U1, opaque cornea only; U2, central anterior synechia; U3, peripheral anterior synechia combined with angle closure; and U4, aniridia or lens anomaly. The opacity appearance and corneal vascularization density observed in slit-lamp photographs were assigned grades according to previous studies. The extent of vascularization was also recorded. The corresponding intraocular anomaly classifications and ocular surface lesion severity were analysed.
Results: Among 81 eyes (65 patients), 41 (50.6%) were right eyes, and 40 (49.4%) were left eyes. The median age at examination was 6.91 months (n = 81, 1.00, 34.00). Two (2.5%) of the 81 eyes were classified as U1, 20 (24.7%) as U2, 22 (27.2%) as U3a, 11 (13.6%) as U3b and 26 (32.1%) as U4. Bilateral CCO eyes had more severe UBM classifications (P = 0.019), more severe dysgenesis (P = 0.012) and a larger angle closure (P = 0.009). Eyes with more severe UBM classifications had higher opacity grades (P = 0.003) and vascularization grades (P = 0.014) and a larger vascularization extent (P = 0.001). Eyes with dysgenesis had higher haze grades (P = 0.012) and more severe vascularization (P = 0.003 for density; P = 0.008 for extent), while the angle closure range was related to haze grade (P = 0.013) and vascularization extent (P = 0.003).
Conclusions: This classification method based on UBM and slit-lamp photography findings in the eyes of CCO infants and toddlers can truly reflect the degree of abnormality of the ocular surface and anterior segment and is correlated with the severity of ocular surface anomalies. This method might provide meaningful guidance for surgical procedure design and prognostic determinations for keratoplasty in CCO eyes.
Keywords: Congenital abnormalities; Cornea diseases; Corneal opacity; Ultrasound Biomicroscopy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
