

Prognostic evaluation of quick sequential organ failure assessment score in ICU patients with sepsis across different income settings
- PMID: 38263076
- PMCID: PMC10804657
- DOI: 10.1186/s13054-024-04804-7
Prognostic evaluation of quick sequential organ failure assessment score in ICU patients with sepsis across different income settings
Abstract
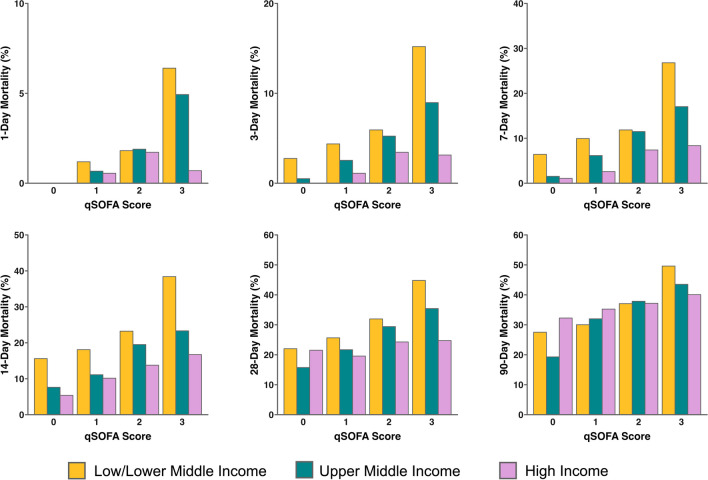
Background: There is conflicting evidence on association between quick sequential organ failure assessment (qSOFA) and sepsis mortality in ICU patients. The primary aim of this study was to determine the association between qSOFA and 28-day mortality in ICU patients admitted for sepsis. Association of qSOFA with early (3-day), medium (28-day), late (90-day) mortality was assessed in low and lower middle income (LLMIC), upper middle income (UMIC) and high income (HIC) countries/regions.
Methods: This was a secondary analysis of the MOSAICS II study, an international prospective observational study on sepsis epidemiology in Asian ICUs. Associations between qSOFA at ICU admission and mortality were separately assessed in LLMIC, UMIC and HIC countries/regions. Modified Poisson regression was used to determine the adjusted relative risk (RR) of qSOFA score on mortality at 28 days with adjustments for confounders identified in the MOSAICS II study.
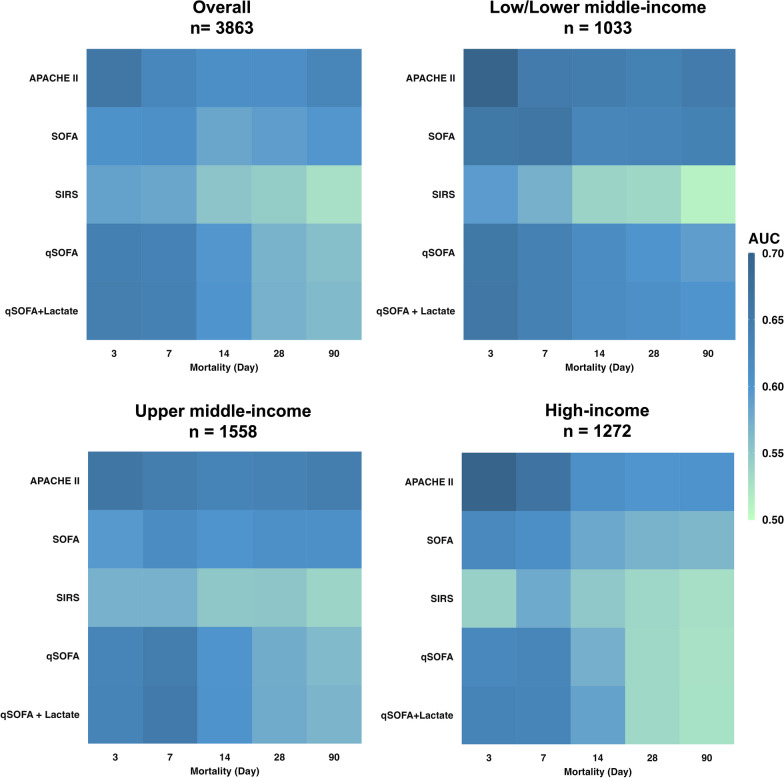
Results: Among the MOSAICS II study cohort of 4980 patients, 4826 patients from 343 ICUs and 22 countries were included in this secondary analysis. Higher qSOFA was associated with increasing 28-day mortality, but this was only observed in LLMIC (p < 0.001) and UMIC (p < 0.001) and not HIC (p = 0.220) countries/regions. Similarly, higher 90-day mortality was associated with increased qSOFA in LLMIC (p < 0.001) and UMIC (p < 0.001) only. In contrast, higher 3-day mortality with increasing qSOFA score was observed across all income countries/regions (p < 0.001). Multivariate analysis showed that qSOFA remained associated with 28-day mortality (adjusted RR 1.09 (1.00-1.18), p = 0.038) even after adjustments for covariates including APACHE II, SOFA, income country/region and administration of antibiotics within 3 h.
Conclusions: qSOFA was independently associated with 28-day mortality in ICU patients admitted for sepsis. In LLMIC and UMIC countries/regions, qSOFA was associated with early to late mortality but only early mortality in HIC countries/regions.
Keywords: APACHE; Critical care; Infection; Mortality; Prediction; qSOFA.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
All authors declare no conflicts of interests.
Figures
Comment in
-
Reflections on epidemiological investigations of sepsis in the Asian Region.Crit Care. 2024 Feb 26;28(1):59. doi: 10.1186/s13054-024-04849-8. Crit Care. 2024. PMID: 38409048 Free PMC article. No abstract available.
-
Limitation of life-sustaining treatments in Asian ICUs: theory versus practice.Crit Care. 2025 Jan 6;29(1):9. doi: 10.1186/s13054-024-05241-2. Crit Care. 2025. PMID: 39762907 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
