

What affects the selection of diverting ileostomy in rectal cancer surgery: a single-center retrospective study
- PMID: 38263089
- PMCID: PMC10804464
- DOI: 10.1186/s12893-024-02316-3
What affects the selection of diverting ileostomy in rectal cancer surgery: a single-center retrospective study
Abstract
Background: The selection of diverting ileostomy (DI) is controversial. This study aimed to explore the factors affecting the selection of diverting ileostomy (DI) following laparoscopic low anterior resection for rectal cancer.
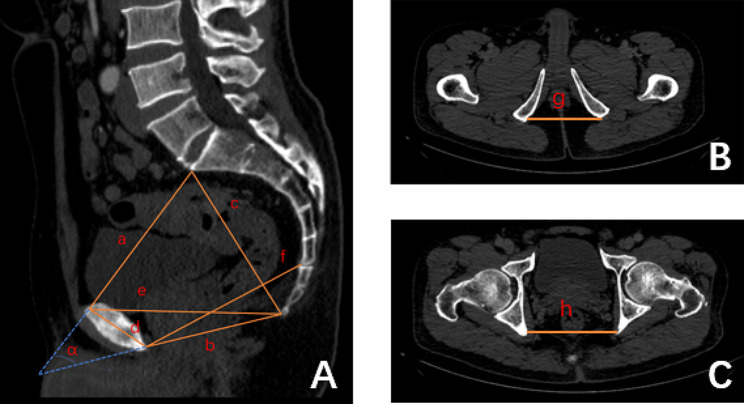
Methods: This retrospective, case-control study included patients who underwent laparoscopic-assisted sphincter-saving surgery for mid-low rectal cancer from January 2019 to June 2021. Univariate and multivariate analyses were performed on the patient's clinicopathological characteristics and pelvic dimensions measured by abdominopelvic electron beam computed tomography.
Results: A total of 382 patients were included in the analysis, of which 182 patients (47.6%) did not undergo DI, and 200 patients (52.4%) underwent DI. The univariate analysis suggested that male sex (p = 0.003), preoperative radiotherapy (p < 0.001), patients with an anastomosis below the levator ani plane (p < 0.001), the intertuberous distance (p < 0.001), the sacrococcygeal distance (p = 0.025), the mid pelvis anteroposterior diameter (p = 0.009), and the interspinous distance (p < 0.001) were associated with performing DI. Multivariate analysis confirmed that preoperative radiotherapy (p = 0.037, odds ratio [OR] = 2.98, 95% confidence interval [CI] = 1.07-8.30), anastomosis below the levator ani plane (p < 0.001, OR = 7.09, 95% CI = 4.13-12.18), and the interspinous distance (p = 0.047, OR = 0.97, 95% CI = 0.93-1.00) were independently associated with performing DI.
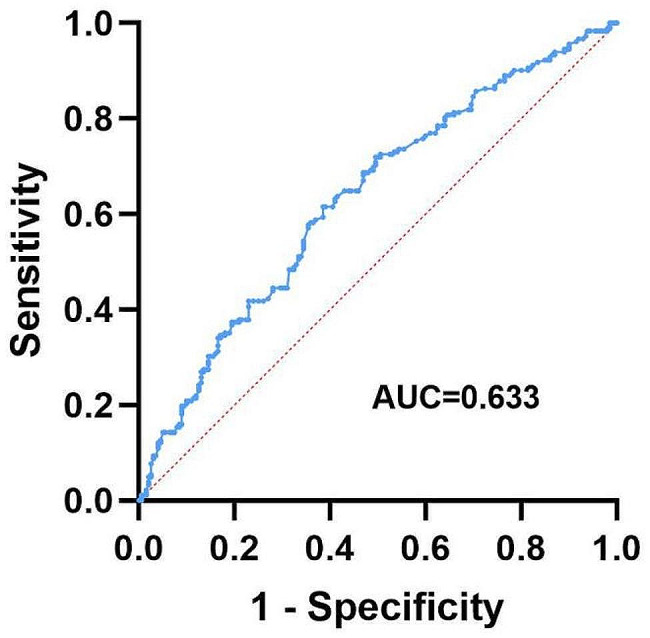
Conclusion: Pelvic parameters also influence the choice of DI. According to this single-center experience, patients with a shorter interspinous distance, particularly narrow pelvic with an interspinous distance of < 94.8 mm, preoperative radiotherapy, and anastomosis below the levator ani plane, prefer to have a DI and should be adequately prepared by the physician.
Keywords: Diverting ileostomy; Laparoscopic surgery; Pelvimetry; Rectal cancer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Who needs diverting ileostomy following laparoscopic low anterior resection in rectal cancer patients? Analysis of 417 patients in a single institute.Surg Endosc. 2020 Feb;34(2):839-846. doi: 10.1007/s00464-019-06837-4. Epub 2019 May 20. Surg Endosc. 2020. PMID: 31111210
-
CT pelvimetry and clinicopathological parameters in evaluation of the technical difficulties in performing open rectal surgery for mid-low rectal cancer.Oncol Lett. 2016 Jan;11(1):31-38. doi: 10.3892/ol.2015.3827. Epub 2015 Oct 26. Oncol Lett. 2016. PMID: 26870163 Free PMC article.
-
[Computed tomography pelvimetry as a predictor of technical difficulty in total mesorectal excision].Zhonghua Wei Chang Wai Ke Za Zhi. 2011 Nov;14(11):846-50. Zhonghua Wei Chang Wai Ke Za Zhi. 2011. PMID: 22116717 Chinese.
-
Diverting ileostomy in laparoscopic rectal cancer surgery: high price of protection.Surg Endosc. 2016 Nov;30(11):4809-4816. doi: 10.1007/s00464-016-4811-3. Epub 2016 Feb 22. Surg Endosc. 2016. PMID: 26902615
-
A meta-analysis of the role of diverting ileostomy after rectal cancer surgery.Int J Colorectal Dis. 2021 Mar;36(3):445-455. doi: 10.1007/s00384-020-03771-z. Epub 2020 Oct 16. Int J Colorectal Dis. 2021. PMID: 33064212 Review.
Cited by
-
Protective ileostomy creation after anterior resection of the rectum (PICARR): a decision-making exploring international survey.Updates Surg. 2025 Jun;77(3):805-823. doi: 10.1007/s13304-025-02111-6. Epub 2025 Mar 23. Updates Surg. 2025. PMID: 40121358
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
