

Synergistic effect of sildenafil combined with controlled hypothermia to alleviate microglial activation after neonatal hypoxia-ischemia in rats
- PMID: 38263116
- PMCID: PMC10804557
- DOI: 10.1186/s12974-024-03022-w
Synergistic effect of sildenafil combined with controlled hypothermia to alleviate microglial activation after neonatal hypoxia-ischemia in rats
Abstract
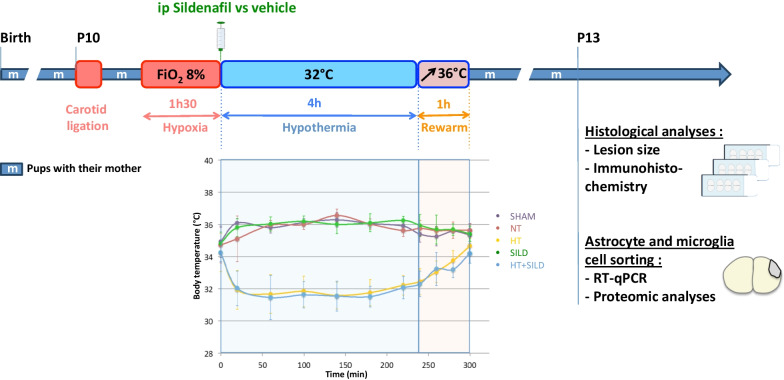
Background and purpose: The only validated treatment to prevent brain damage associated with hypoxia-ischemia (HI) encephalopathy of the newborn is controlled hypothermia with limited benefits. Additional putative neuroprotective drug candidates include sildenafil citrate, a phosphodiesterase-type 5 inhibitor. The main objective of this preclinical study is to assess its ability to reduce HI-induced neuroinflammation, in particular through its potential effect on microglial activation.
Methods: HI was induced in P10 Sprague-Dawley rats by unilateral carotid permanent artery occlusion and hypoxia (HI) and treated by either hypothermia (HT) alone, Sildenafil (Sild) alone or combined treatment (SildHT). Lesion size and glial activation were analyzed by immunohistochemistry, qRT-PCR, and proteomic analyses performed at P13.
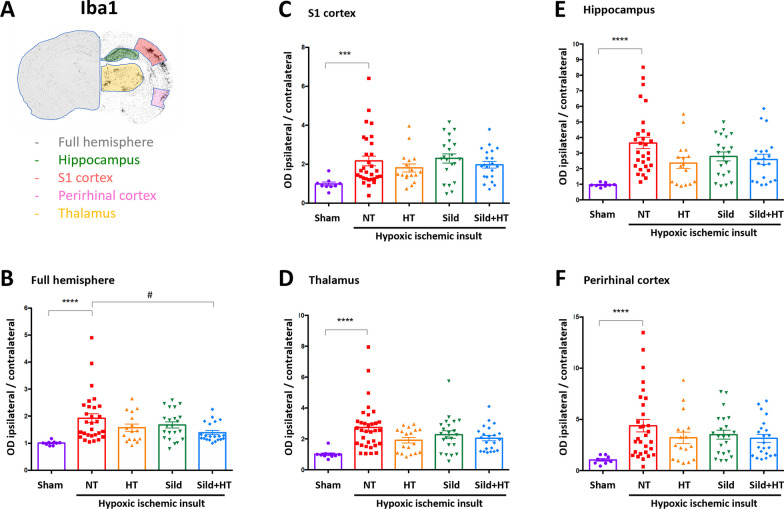
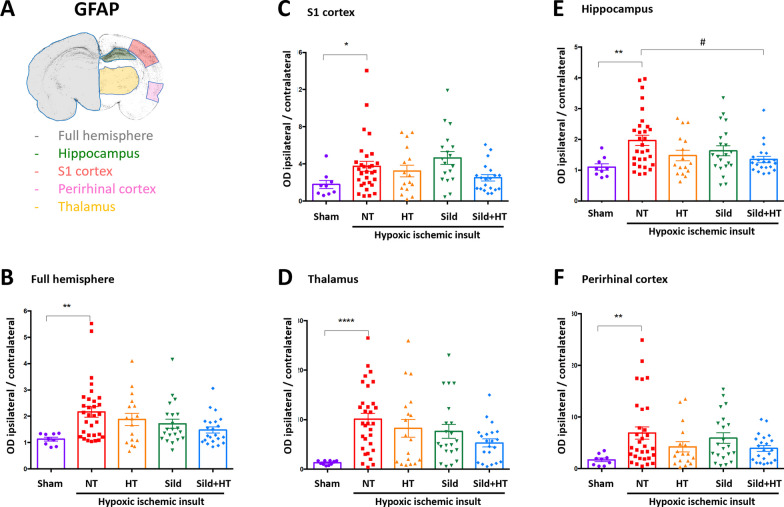
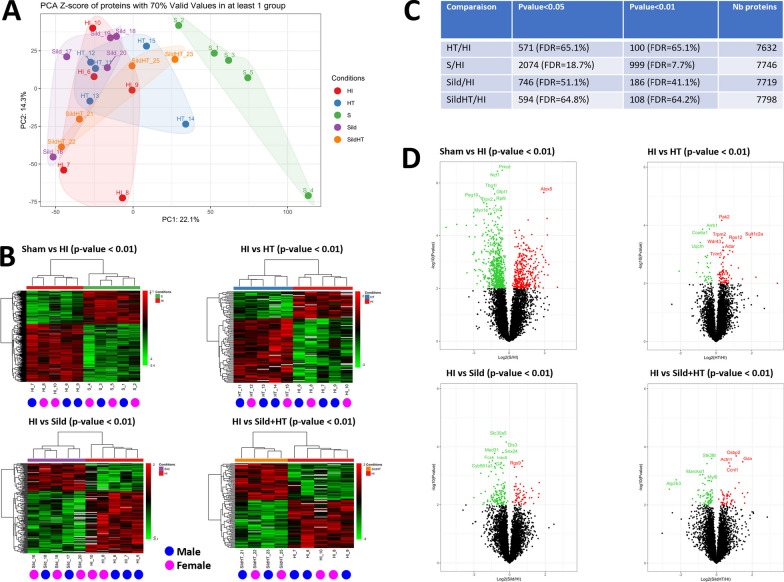
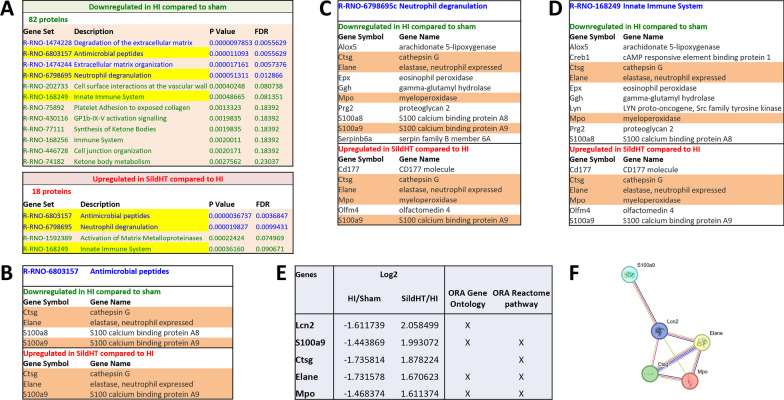
Results: None of the treatments was associated with a significant early reduction in lesion size 72h after HI, despite significant changes in tissue loss distribution. Significant reductions in both Iba1 + (within the ipsilateral hemisphere) and GFAP + cells (within the ipsilateral hippocampus) were observed in SildHT group, but not in the other treatment groups. In microglia-sorted cells, pro-inflammatory markers, i.e. Il1b, Il6, Nos2, and CD86 were significantly downregulated in SildHT treatment group only. These changes were restricted to the ipsilateral hemisphere, were not evidenced in sorted astrocytes, and were not sex dependent. Proteomic analyses in sorted microglia refined the pro-inflammatory effect of HI and confirmed a biologically relevant impact of SildHT on specific molecular pathways including genes related to neutrophilic functions.
Conclusions: Our findings suggest that Sildenafil combined with controlled hypothermia produces maximum effect in mitigating microglial activation induced by HI through complex proteomic regulation. The reduction of neuroinflammation induced by Sildenafil may represent an interesting therapeutic strategy for neonatal neuroprotection.
© 2024. The Author(s).
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures


Similar articles
-
Sildenafil mediates blood-flow redistribution and neuroprotection after neonatal hypoxia-ischemia.Stroke. 2014 Mar;45(3):850-6. doi: 10.1161/STROKEAHA.113.003606. Epub 2014 Jan 28. Stroke. 2014. PMID: 24473179
-
Hypothermia modulates myeloid cell polarization in neonatal hypoxic-ischemic brain injury.J Neuroinflammation. 2021 Nov 13;18(1):266. doi: 10.1186/s12974-021-02314-9. J Neuroinflammation. 2021. PMID: 34772426 Free PMC article.
-
Sildenafil improves hippocampal brain injuries and restores neuronal development after neonatal hypoxia-ischemia in male rat pups.Sci Rep. 2021 Nov 11;11(1):22046. doi: 10.1038/s41598-021-01097-6. Sci Rep. 2021. PMID: 34764335 Free PMC article.
-
Sildenafil, a cyclic GMP phosphodiesterase inhibitor, induces microglial modulation after focal ischemia in the neonatal mouse brain.J Neuroinflammation. 2016 Apr 28;13(1):95. doi: 10.1186/s12974-016-0560-4. J Neuroinflammation. 2016. PMID: 27126393 Free PMC article.
-
Early Neuroprotective Effects of Bovine Lactoferrin Associated with Hypothermia after Neonatal Brain Hypoxia-Ischemia in Rats.Int J Mol Sci. 2023 Oct 25;24(21):15583. doi: 10.3390/ijms242115583. Int J Mol Sci. 2023. PMID: 37958562 Free PMC article.
Cited by
-
Single-Cell Transcriptomic Profiling of Brain Cells in Newborn Rats Following Hypoxic Ischemic Encephalopathy.FASEB J. 2025 Aug 31;39(16):e70929. doi: 10.1096/fj.202402891RR. FASEB J. 2025. PMID: 40799188 Free PMC article.
-
Identification and verification of key molecules in the epileptogenic process of focal cortical dysplasia.Metab Brain Dis. 2024 Nov 29;40(1):47. doi: 10.1007/s11011-024-01426-4. Metab Brain Dis. 2024. PMID: 39612062
References
-
- Edwards AD, Brocklehurst P, Gunn AJ, Halliday H, Juszczak E, Levene M, Strohm B, Thoresen M, Whitelaw A, Azzopardi D. Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: synthesis and meta-analysis of trial data. BMJ. 2010;340:c363. doi: 10.1136/bmj.c363. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
