

Distinguishing sterile inflammation from graft infection
- PMID: 38263206
- PMCID: PMC10804788
- DOI: 10.1186/s13019-024-02504-5
Distinguishing sterile inflammation from graft infection
Abstract
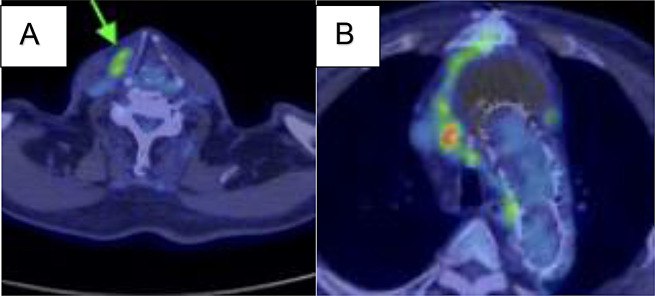
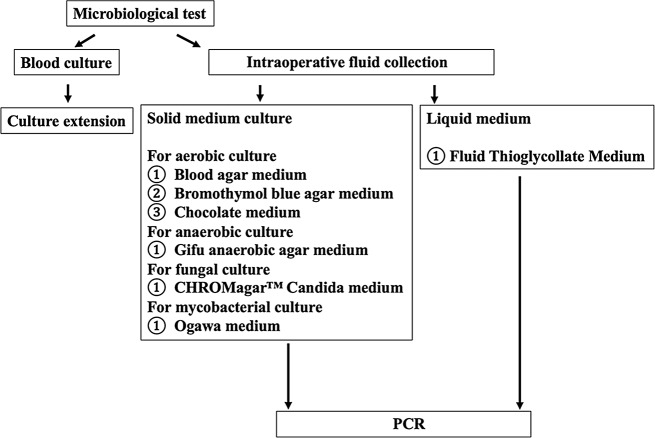
We describe the case of a 68-year-old man who underwent ascending aortic replacement and thoracic endovascular aortic repair. Four years later, the patient developed neck pain on the right side and chest computed tomography showed expansion of fluid in the mediastinum which had extended to the neck. Echocardiography revealed advanced severity of aortic regurgitation and decreased ejection fraction. Given the progression of aortic regurgitation, decreased cardiac function, and rapidly expanding fluid accumulation causing neck pain, reoperation was indicated. All microbiological test including polymerase chain reaction were negative indicating absence of any infection. The patient is being followed-up without antibiotics and CT has not shown peri-graft fluid 2 years postoperatively. Since infection cannot be excluded completely, it is important to assess the condition with selective medium, extended culture periods, genetic testing, and consultations with microbiology laboratories when normal culture tests for general bacteria, and fungi are negative which can help avoid drug-resistant bacteria count, elevated medical costs, and drug side effects due to the improper use of antibiotics through proper diagnosis.
Keywords: Fluid collection; Graft infection; Inflammation; Non-bacterial; Peri-graft; Sterile.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Williamson MR, Boyd CM, Shah HR. Prosthetic vascular graft infections: diagnosis and treatment. Crit Rev Diagn Imaging. 1989;29(2):181–213. - PubMed
-
- Holliday RA, Prendergast NC. Imaging inflammatory processes of the oral cavity and suprahyoid neck. Oral Maxillofac Surg Clin North Am. 1992;4(1):215–40. doi: 10.1016/S1042-3699(20)30578-1. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
